snakemedic
-
Posts
26 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Everything posted by snakemedic
-
You can get about a gazillion index cards for 5 bucks or so...a lot of the learning is in the making...don't cheat yourself out of it. Dwayne I think this says it all. After 15 years I'm still learning and relearning. Snake
-
contrary to popular opinion, even ontario shops out calls turned down to weather. Medics need to stand up for themselves and "refuse to be abused". Still, very saddened by this tragic news. Snake
-
TRAUMA - Episode 12, March 15
snakemedic replied to Suburban/Rural Medic's topic in General EMS Discussion
I'm glad I'm not the only one that caught that, shameful act of "heroism". I don't know what was worse, the poor history on the anaphylaxis which apparently needed the use of a BVM after the administration of epi? I guess she was in extremes, what ever I began getting turned off quickly at that point, then let's walk the cardiac patient out to the ambulance....did they not bring the cardiac monitor to the back for the "short of breatch" patient but the above quote put me over the edge too. I don't think this promotes the profession and actually does a lot to take away from a lot of time and effort many paramedics have put into becoming very highly trained.....perhaps this is an anamoly of all paramedics and only reflects San Fran's medics or at least how they wish to be portrayed. I will not watch this ever again....two thumbs down. Jake -
things that i never thought i would have to.....
snakemedic replied to 2wheelinemt's topic in Archives
We pray the Lord brings people around you to strengthen you in your weak times and to walk with you in your struggles. You and your family are in our thoughts and prayers . Snake -
I am sorry that you had such a crappy shift, I think the hardest thing to do is not take it out on those we love or those who call us for help. You did well reaching out and you received a lot of great support. All the best, Snake
-
I have noticed over the past 8 years that intubations have continued to go down and I think the numbers also go down because we become a little more mature and confident in managing the airway with other adjuncts first, however mine have dwindled to: 3 facilitated 2 of which were accomplished on second attempt 2 RSI accomplished on 1st attempt. An adjunct I've noticed that made a big difference for me was the Bougie, never had one until I went to the air environment, love it. and 6 intubations in the OR during CME 1st attempts each but all patients stable and healthy elective surgery. Snake
-
Any help with learning phases 0-4?
snakemedic replied to Jeepluv77's topic in Education and Training



-
To answer your question of giving NTG without IV, I would say if that is the road you are persuing then yes, I would be comfortable giving NTG without IV. Her sysstolic is 110 and her map acceptable to give nitro. How did she respond to her own ntg, did she fall on the floor? Her chest is clear so if you need to lay her down because she drops her pressure you can do that. This stuff is not etched in stone, you need to think about what your trying to accomplish, take the workload off the heart, but , don't increase the MVO2 by dropping the pressure to far (risk/benefit). If it was her first time ever with NTG I would be more concerned with a possible pressure dump but....that's what they pay you to do, think. I would stay away from the MSO4 until having a line the concurrent histamine release might be more deleterious than uselful. In the end try to do the best you can for the patient like they were your own family. Out of curiosity, did you ask the Dr what they think about the NTG without a line? Snake
-
Any help with learning phases 0-4?
snakemedic replied to Jeepluv77's topic in Education and Training
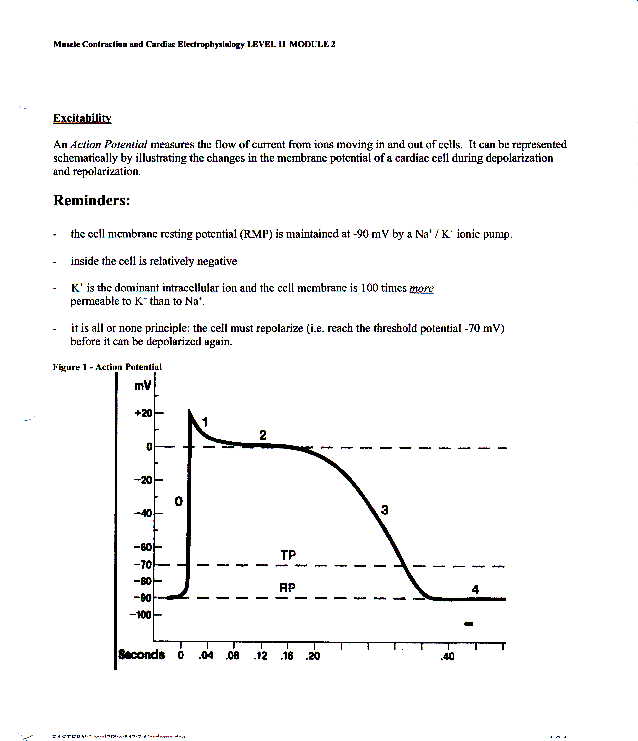
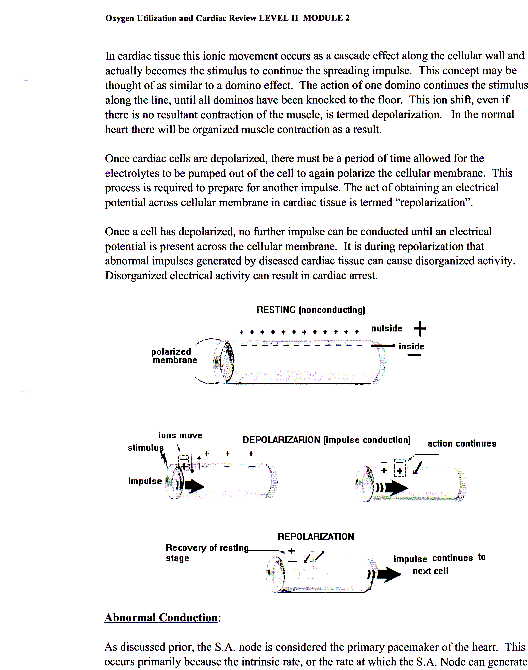
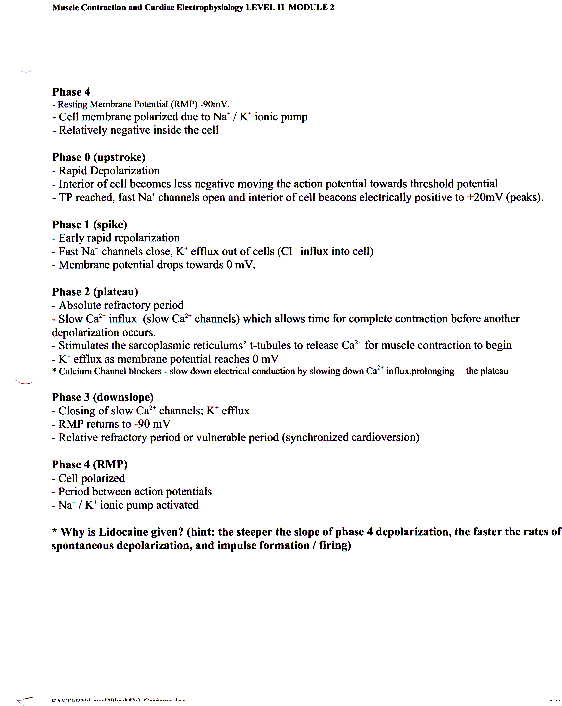
Hey there, this is very basic and I will add a file here in the next two days of a good diagram you can use as a visual learner. It takes some time to grasp the concept. remember whats in the cell and outside the cell in a normal homeostatic state. Na+: Sodium is outside K+: Potassium inside Ca++: outside think of a concentration gradient as a slide, so "things" slide down the concentration gradient from positive to negative. Phase 0: Na+ slides in Phase 1: Na+ lets Ca++ slide in Phase 2: K+ slides out Phase 3: K+ slides out (remember at about -70 mV the cell hits the relative refractory period where some cells will depolarize (VF?) Phase 4: Na+/K+ ATPase pump is very strong when supplied with energy (a body building dad) so it pushes his children Na+ and K+ up the slide ( Na+ now pushed outside cell, K+ pushed inside the cell...but he favors one kid, look up which one.) Sorry it's rudimentary I'll send a little better in a few days, this covers the basics for you. Keep this infront of you when your looking at your cardiac drugs and it will give you a good idea of why Lidocaine and Amio are used in ACLS. make the cell more positive, it has the tendancy to depolarize easily make the cell more negative, it has the tendancy not to depolarize as easily Let me know if this helps. If your more interested in pharmacology, I would suggest investing in Lippincott's it has helped me through all my education needs thus far. Best of luck Snake -
I read someone spoke of ORNGE....don't hold your breath about the takeover and grand plans just yet....wait and see how it all plays out first. pay your pilots a salary not by mile or call and just ask them to do a weather check. Keep it safe.
-
Have fun, take a little time each day to study and realize none of us have all the answers. Good luck and congrats. Jake
-
Would you ALS or BLS this patient and why?
snakemedic replied to Arizonaffcep's topic in General EMS Discussion
I don't know folks, you have a patient who is stable, BLS on scene and no ALS on scene and a stab to the chest/back. The patient needs a trauma center, and he may need surgery. The Canadians on this form have it right, start to transport and if you can rendezvous with Als but do not delay transport. The most that ALS will do is IV/ decompress even still, accellerator therapy remains treatment of choice. I would BLS if no ALS on scene....and I certainly wouldn't take my direction from a nurse on the other end of a phone, your job is to make deciscions and be a patient advocate....he needs the trauma unit and surgery. Jake -
Well, quite honestly I think some of you think too highly of yourselves on this form. I dare not speak like that about dust because I've often read his posts and he is bang on 99% of the time, but guys, stop eating our young, some of you live and die being called a medic, it's a damn job, a career but it isn't who you are. As for the person asking the original question, find the way that works best for you and where you are in life right now. The books I would recommend are :lippincott professional guide to pathophysiology, springhouse professional guide to diseases, tintinalli emergency medicine just the facts, lippincott pharmacology, lippincotts medical physiology principles for clinical medicine, jones and bartlett 12 lead ecg the art of interpretation. On top of those find a good nursing book on medical math and practice practice practice. Qcards are great to keep with you for medications and quick notes that you can review on the fly at work or home. Bring a little book with you and write down questions you have and then look them up on the internet or emt city or books. Ask your patients about the disease processes they have, how it affects them etc. Apart from that if you are looking for more and a good place to start without buying books, email me at snakemedic18stn@yahoo.ca and I will send you all kinds of stuff to get you off and running and build you up rather than throwing you to the wolves. my humble opinion snake
-
He's a paraplegic and has a foley catheter, why are we standing him up and then mentioning he is quite uncoordinated. Apart from that, what is the color of his urine, when was it last changed, when was it last drained and how much, what time of the day is it, how long a paraplegic. How much has he vomited up?
-
you got the tube, congrats, everything else is academic. If you ever get a chance read wallis book on emergency airway management and consider taking his course.
-
I agree with you to some extent Dust, I think just throwing 'stuff' out to give the perception of more ability is misleading but it is also insulting. Your Bls today are the ALS of the future and I think we can all agree that the more knowledge base you have to draw on the better prepared you are to do your job well. I think the best service you could provide to your BLS is deeper knowledge base and then add the skills later.
-
Please forgive me if this has already been mentioned but another "last ditch effort" might be to consider stop ventilations altogether after he arrests and some chest pressure to try to alleviate some of the air trapping, another option is blateral needle decompression, but in saying this, most of us have been there, hind sight is 20/20 and this is all academic after the fact. The best thing you can do is take all the great suggestions folks have offered and add it to that bag of tricks you have and draw on it next time. Sounds like you did great and you didn't fool around GOOD JOB!
-
well, logic would dictate that you use your health classes to teach all your students once a year with refreshers periodically (ie plug in the pads) and professional developement days to train all your teachers and janitors, and good gracious it probably wouldn't take long until everyone is familiar with it. Just a thought but my defib never works, they all end up dead;)
-
Lippincott's Illustrated Reviews : Pharmacology : Special Millennium Update Mary J Mycek, Richard A Harvey, Pamela C Champe It starts right from square one and takes you through the receptors and reasons the drug classes work, then from there you may go to better understand how individual drugs work. Always remember even for AlS road paramedics....a deep knowledge is great but the best als always starts with good bls. ask your education department, they should be more than happy to assist you.
-
To all the new members who haven't introduced themselves yet
snakemedic replied to Just Plain Ruff's topic in Meet and Greet
Hey, I'm Jake, working in Toronto just shy 10 years now, currently living at 40 station with all the other homeless street folks, psychs, drunks and generally unwell people of the big smoke....and loving it.....well, sometimes. -
ASA is contraindicated in asthmatics unless they have taken ASA with 'no adverse reactions' (as per Medical Directives) As for the pregnancy and ASA, I think it was said eariler; risk vs benefit and if you are going to call the base hospital realize that it is a crap shoot and depending on the recent literature that the MD who picks up the patch line has been reading will determine weather or not you get your order....I have also been told "NO ASA and NO NITRO" but that being said you have to know the doc in question also...like I said, it's a crap shoot. "keep yourself up to date and keep learning, it can only benefit the pt."