BoCat9
-
Posts
64 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Everything posted by BoCat9
-
Seems like the year has crept by and I wanted it to speed up. Now the days are flying by and I wish thy would last longer. Test on the 2nd and the 8th, both are scaring the crap outta me.
-
Considering the recent surgery and the immobilization of the leg, I would look for a possible DVT and/or pulmonary embolus.Is there any swelling in the rt leg? I would consider Lasix for the pulmonary edema and Romazicon for the benzo overdose. Also I would consider RSI to protect the airway.
-
I know a majority of 911 calls are going to be someone wanting a ride to the ER, but there will be some emergency situations. My main thing is the act that for the past 5 years, I haven't really used my skills. I take vital signs, do my assessment and then there is nothing else I can do. By the time I see them, any interventions have been done. I don't get the opportunity to see a trauma patient and do the splinting or put someone on the backboard. I still enjoy this line of work, I'm just bored with doing the same thing over and over again. Most of my day is taking someone from the hospital to rehab or to the nursing home. Biggest thing I do on a regular basis is put someone on O2. On long transports I go through "worst-case" scenarios with the person I am transporting and think of things I will do if something happens. I just want the opportunity to do different things. Quote 2) Considering that I'll (hopefully) be a medic next month, which side is it better to work on starting out as a medic? Obviously the change will be good- new challenges, new responsibilities, etc. Not sure the "side" you are referring to here. IFT or 911
-
I have been an EMT for almost 5 years, and I ave been doing transport work the whole time. I enjoyed it at first, getting to know the people and their families and enjoyed the work. I am really starting to get fed-up with it now though. I am starting to be irritable even before I get to work. I have started to snap at my co-workers and my partner and coworkers can tell I am tense. I've even started having nightmares and trouble sleeping, esp the night before my shift. I am afraid I am beginning to burn out. I am starting to look for 911 work and just have a few questions. 1) How hard is it to get out of the "transport" state of mind and into the "911" state? 2) Considering that I'll (hopefully) be a medic next month, which side is it better to work on starting out as a medic? 3) Does anyone know of any services that do both 911 and transport in the USA? I am looking into moving at some point in the next year and a "dual" service may help to ease the transition. Thanks for you time. Bo Edited for a grammatical error.
-
i would like to thank all of the men and women who have fought for the freedom of me and everyone else in this country.
-
I have one month and 2 days until my practical testing and I'm getting nervous. Any tips on how to relax about it and prepare the best I can?
-
Ok, two quick questions about stabilization. Can a flail segment safely and effectively be stabilized using a KED? My partner said it could, but just wanted to get other input. Also, I was told in class not to use sandbags, IV bags or anything heavy due to the fact it will cause respiratory difficulty or make it worse. Are sandbags still an accepted practice, or is it best to use bulky dressings? Thanks for looking. Bo
-
Two modules left in class, Operations and review. Then the alphabet classes. I feel good about it in the fact I think I'll pass the class and get my medic. Is it normal to get extremely nervous about what will happen after you get your medic? I am feeling that way right now, have been for a week. I keep thinking about what will happen when I get my first true ALS call. What if I forget something and the patient dies? What if I mess up?
-
Ok, I'm sorry that I am not medic and cannot administer pain medications, but what I am trying to say is that instead of waiting on scene for 15 minutes or more for a medic who can take care of them to a higher level than I can, I will make them ans comfortable as I can and cut the time they have to wait. If the intercept is 15 minutes away and I meet them halfway, it will take 5 min or more the patient will have to deal with the pain. Sure it would have been better to have sent out a ALS unit out in the first place, but sometimes that is not possible or just not done. I do the best I can with my scope of practice.
-
They will be waiting just as long or longer if I stay on scene and wait for a medic. I work transport and in most cases neither me or my partner knows the area. I have the number to the areas we go to regularly, but I don't know the numbers to all the places we go to. It's not for direction, I will stop and ask for directions to a street before I tie up a 911 line. This is for an intercept if my patient goes downhill on me.
-
I have had one call where I have asked for an ALS intercept, really didn't need one and then a couple where I needed one and didn't ask for it. I have also had times where my partner cancelled the ALS I had coming to me and then told me to ride the call, but I digress. I have started looking at the situations my patient has. If it is something that could benefit from ALS interventions I will look a the distance to the hospital that the patient is going to go to. In almost all cases I won't wait around on scene. If I can be at the hospital before the unit will be able to get to me, I will do what I can and not really even call for another unit. If I will have an extended transport, I will have the intercept meet me en route so it will cut the time to definitive treatment. I have also been told that if a patient I am transporting goes downhill and I ave absolutely no idea where I am that I should 911.
-
Well, I passed Trauma with an 88. Special Considerations for a few weeks. Drug calculations test next week, so I really need to practice those, esp the Dopamine and Lidocaine drips.
-
Look for one with a fairly short thick tubing. I've tried a lot of different ones and I can hear the best with that kind. Also try using the "mushroom" shaped earpieces, they will fill your ears better and filter out a lot more background sounds.
-
No pacemakers or anything like that. According to my instructor, the guy who actually talked to the nurse, they did an ultrasound and a dopplar. The only places they saw any blood moving was in the brachial and carotid arteries. No heart sounds at all. No chest x-ray was done. They are doing an autopsy though. The guy was unresponsive, he would only sit up for a second or two before he went back down. Initially I asked if they were checking a pulse with their thumbs, the instructor said "I hope not." Shot it the wind, but possible.
-
Ok, a little more info. Heart sounds were never heard. Pulse was during CPR and without CPR. No known medical hx. This is coming from the nurse at the hospital that worked on the pt. I really don't know what to think either and everyone has told me its not possible. Please remember I was not on this case and I am giving you the facts as presented to the class.
-
Ok, a case was presented to us in class, actual call that took place sometime last week. We were told we could use any source to find the answer. Ambulance service brings a mid-50 y.o.m. into the hospital. Found pt unresponsive, put pt on the monitor showing asystole. Crew checked a pulse, found a pulse in the carotid and brachial pulse. Pt cyanotic from nipple line up. HR ranged from 70-200, erratic. Pt had a BP or 110/70-200 systolic. Pupils dilated, nonreactive. Agonal resp, medics tubed the pt. Pt placed on 3 different monitors, leads and pads changed with the monitor. I monitor on the back of the ambulance, 2 monitors in the hospital. Hospital staff continued to work the pt for an hour and a half, each time they stopped to pronounce him, he would sit up, look around and then lay back down. Has anyone ever heard of this happening or have any idea what may have caused this?
-
Well, finally getting the hang of the IV's, so I'm happy. And I passed medical module 2 with a 100. Over the hump and now I'm feeling like I may get through this year! Woo hoo! Just thought I would give you an update. Trauma up next.
-
I was on a routine transport once and was taking a set of vitals and found out the cuff I was using had a broken gauge. I asked my partner to remind me to get another one before our next call, and she said "why, I'm not going to take any anyways". I lost any trust I had in her that day.
-
OK, I'm having problems with IV's. I can mainly get them in class and on people that let me use them as guinea pigs, but on my patients, I have a lot of problems. I got one on my first ride along day, but I have missed every one since, except the one I hit a valve on. It's really starting to irritate me. Maybe I just get nervous or something. Any advice?
-
Metaprolol can mask the early symptoms of hypoglycemia. Name 2 or more uses for the KED.
-
I'll put it like my boss told my coworkers and me at a meeting. "I would like for you all to have a lunch break and we will try to make that happen, but sometimes it is not possible." We were also told to bring something small with us. Have a pack of nabs or even bring a sandwich with you. It will help tide you over until you can get something more substantial. Only worry I have is when my partner is a diabetic and we don't get a chance to stop. Peace...
-
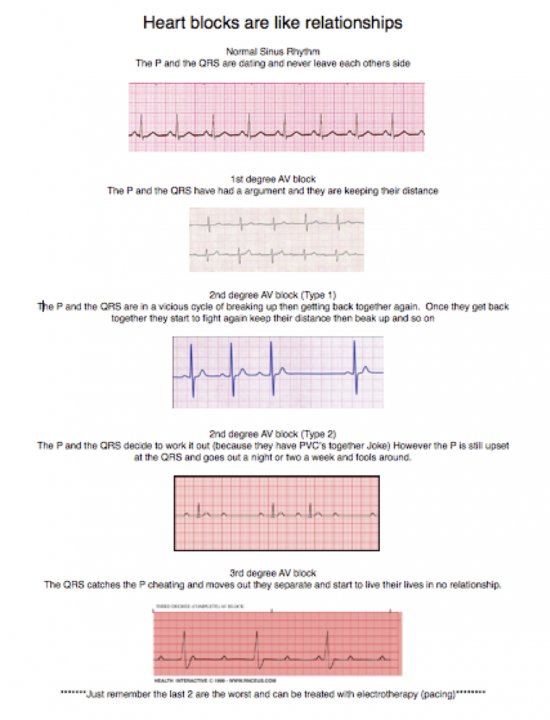
Found this on facebook, under paramedic tips and tricks, thought it was interesting...

-
Try some scenarios, esp. the things that you encounter most in your area. It may be that she freezes when she gets on scene and she just needs the practice in verbalizing what she is going to do. If you can go this far, maybe have someone play the part of a pt on a easy day. Actually have her do some things. Let her take the lead, some people just need that push. During my ride time, the medic on the truck said, on a stable pt, that both he and his partner were going to stand back and let me question the pt and do my assessment. Then the medic would ask me what I want to do, and as long as my treatment wouldn't be detrimental to the pt or totally off the wall, that is what the treatment would be. Then after the call he would ask me how I felt it went and then he would give me his feelings about it. Some people are just shy and need the push in order to get them jump started. Also talk to your superior and see if she could ride third some in order to get her used to being on scene. If so, have the crew chief sit down with her and tell her his/her expectations. That way she knows, "OK, I will be doing this on the calls unless told otherwise." Hope this helps.