


Ace844
-
Posts
1,350 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by Ace844
-
-
Pt. denies using any drugs, or ingesting anything toxic.
what does reciprocial mean?
Reciprocal changes occur on a 12-lead in 'opposite' leads. So if there is elevation in a few leads, there will be depression in the 'opposite' leads. As far as the scene, i thought soemone had asked that, but in case not, add that to the list, and as well whatever other bystander, partmner, PD, etc.. info you can get or see.
-
ok, when you isolate the kid from the parent, any further tox related information coem out? Is the pt a smoker? supplement user? Any signs of Drug abuse-use?What activities was she partaking in prior to coming home, running exertional, etc...? Next, since you didnt mention it, Breath sounds, what are the other B/P's, etc...? Any murmurs?
-
Pt. is on 02, as requested with no relief
How about the rest of the H&P-P/E? Is the depression reciprocial, any axis deviation, any question of recnt tox or substance ingestion?
-
PMHX, Meds, ALL, V/S's,complete head to toe assessment, and Events preceeding, v/s's including bilat B/P's pulse ox, 12-lead, and pert + and - cardio-respritory exam findings.
Thanks,
ACE844
-
"GA,"
It's called ADVOCACY...Contact PRPG and or CAPEM; and they can put your preaching to work...where you will be doing more than just taking up space on a forum..
ACE
-
Go to www.pandemicflu.gov --- everything I have stated is fact, and will make it's way to you soon. Our public health agency is taking great pains to educate ems, fire, and PD to this upcoming threat. I imagine other states will do so also.
Kindly refer yourself to my previous posts.....
ACE844
-
IF we are about saving lives, then we should be involved in the things that save lives, just as firefighters are involved in building code. If we do not push for CPR and AED placement, who will ? And dead doesnt have to be dead if CPR is started sooner and an AED is available.
As far as RSI, I agree with you, but our intubation failures are due to inadequate training, which is something that could be fixed. How many departments have REAL training every month, versus some canned pencil-whipped program where you just shuffle some papers to meet requirements.
The value of lab work: Knowing the white count of someone with a fever, knowing the H&H of a trauma patient shortly after incident, knowing the calcium, potassium, and magnesium level on your dialysis patient, being able to do cardiac enzymes on a chest pain patient -- would it change what you do now, maybe maybe not ? Could it open new treatment doors, yes ?
Computers can open a variety of doors besides patient reporting. You can load programs that improve safety -- such as Pharmaceutical Reference Guides, Haz-Mat/Cameo Programs. You can improve intradepartmental communication, dispatch capabilities, and probably several more things.
Trauma -- no we cant do surgery, but how many people still have to wait to long for an ambulance, or do not have access to a trauma center ? Have we significantly improved the golden hour
AGAIN, KINDLY DO A SEARCH, THOSE DISCUSSIONS HAVE OCCURED, AND THE INFORMATION IS AVAILABLE!! If you'd like to post those seperately in the applicable threads, thats one thing...this is preaching from a pulpit..
ACE844
-
GA
Sorry, I didn't misunderstand what was reported. I just included the links so people could read the articles for informational purposes. I was not advocating there is a vaccine, just reporting what I read.
I think he was trying to talk at us again with no room for discourse, and or made a vague personal attack as he posted right below me...either way, this poster needs to stow the pulpit..
ACE
-
"GAMedic,"
The evidence and information as "JPINFV," has taken the time to point out to you is ALREADY HERE. My suggestion is to do a search and leave the preaching for whatever religeous or public platform you prefer. There are many posts here to which are still awaiting your reply with evidence and actual factual information. Until then, good luck and have a nice day,
ACE844
-
You must have misunderstood what was reported about a vaccine. I attended a conference on this subject this month, and the epidemiologist stated that a vaccine could not be developed until about 6-8 months after the virus crossed over to humans. That has occured in central Asia, so a vaccine may be available for that particular strain. That will not do any good for anyone who gets it in the future, as the virus will change by then. Everyone should read up on this one, as it will kill more 20-40 year olds than the previous flus due to the immune system issues that were mentioned above (usually children and elderly are hit worse). The flu of the early 1900s killed 600 million people world-wide, the experts are predicting this one to be far worse.
"GAMEDIC,"
I am going to say this once, and politely. Kindly don't tell me what I do and don't understand because as you can see I was the one who posted the majority of the information here about this. Also, based on your posts it appears to be YOU who needs to evaluate what is and isn't understood in your world. There are a number of threads initiated on this board which are awaiting your replies to overwhelming evidence which contradict the things you have posted and reported as fact. So in closing, until you post facts, and answer the other posts with verifiable and 'reputable' information, don't come here and preach to me about what I do and don't understand..Here's your:

OUT HERE,
ACE844
-
 I only answer because I respect your opinions mostly vs-eh?, and think maybe you're going somewhere with this....Plus I love to watch these arguments unfold...
I only answer because I respect your opinions mostly vs-eh?, and think maybe you're going somewhere with this....Plus I love to watch these arguments unfold...I believe in a higher being.
I don't believe my definition of a higher being fits everyone or even anyone else.
And nope, I'm not here to sell this to you.
This works for me, I hope your way works for you.....
Dwayne
God and I are buddies....
Yeah..what he said....
 above....and yes god and I have a very special relationship... :shock: 8)
above....and yes god and I have a very special relationship... :shock: 8) [stream:375f0dc0ad]http://www.moviesoundscentral.com/sounds/full_metal_jacket/god.wav[/stream:375f0dc0ad]


Out Here,

-
-
Yeah, forget any care at all....SHTUFF....My AVATAR SAYS IT ALL "GOT SHOES LADY!!"
-
Hello Everyone,
At various times on this board we have had proposals to chnage the state of EMS and an oft asked question is how. While doing some reading I stumbled upon this article which we ALL should read and I think it could give us each a basic idea and frame work for which to perform some organized EMS lobbying from, then begin to effect soem much needed changes.
Hope this Helps,
ACE844
http://www.imedicine.com/DisplayTopic.asp?...3&topic=689 ; How to Lobby EffectivelyEmergency Medicine - Legal Aspects Of Emergency Medicine ; Author: Dan K Morhaim, MD , Member, Maryland House of Delegates 1994-2006; Consulting Staff, Department of Emergency Medicine, Sinai Hospital of Baltimore; Faculty, Johns Hopkins School of Public Health
Editor(s): Richard Lavely, MD, JD, MS, MPH , Lecturer in Health Policy and Administration, Department of Public Health, Yale University School of Medicine; Francisco Talavera, PharmD, PhD , Senior Pharmacy Editor, eMedicine; Matthew M Rice, MD, JD , Vice President, Chief Medical Officer, Northwest Emergency Physicians, Assistant Clinical Professor of Medicine, University of Washington at Seattle; Assistant Clinical Professor, Uniformed Services University of Health Sciences; John Halamka, MD , Chief Information Officer, CareGroup Healthcare System, Assistant Professor of Medicine, Department of Emergency Medicine, Beth Israel Deaconess Medical Center; Assistant Professor of Medicine, Harvard Medical School; and Craig Feied, MD, FACEP, FAAEM, FACPh , Director, National Institute for Medical Informatics, Director, Federal Project ER One, Director of Informatics, Washington National Medical Center, Director, National Center for Emergency Medicine Informatics"]
Politics is important to medicine because of the myriad ways it influences medical practice. Malpractice, graduate medical education, Medicaid reform, managed care rules, Consolidated Omnibus Budget Reconciliation Act (COBRA), "prudent lay person" bills, hospital financing, and occupational safety are just a few of the ways government directly influences emergency medicine. In today's highly charged political and medical climate, emergency physicians must participate in governmental process.
Nearly every important government action influences emergency medicine indirectly because many patient visits to the emergency department (ED) are precipitated by social problems that may be caused or alleviated by government action.
Government is not an abstraction; governments are made of people. The legislators who comprise government are usually responsive to their constituents. The closer the legislator is to voters, the more responsive the legislator. Therefore, state legislators are easier to reach than are federal representatives. However, most issues key to emergency medicine are decided at the state level.
Physicians in general are regarded as a knowledgeable and influential group, and ED physicians have a special ability to influence the political process because most legislators know that ED physicians see and treat patients regardless of the patients' ability to pay. Although most legislators are now aware that EDs provide a vital social and health safety net, many legislators still need to be educated about the basics of the medical profession.
The political process is, by nature, a responsive one. The problem is that the political process responds only to input that is received, and very rarely do legislators actively seek alternative views. Many citizens are predisposed to the cynical notion that politicians are bought and sold, and many citizens believe that the average citizen has little or no influence. In reality, the ability for an individual citizen to influence politics is substantial, but like all other tasks, it requires patience, practice, and persistence.
Several simple guidelines make any physician a more effective lobbyist at the local, state, or federal level.
Do not give up
"If at first you don't succeed, try, try again." Many bills take years to pass. Legislators are bombarded by competing views, and sorting out the issues takes time. Even seasoned legislators become frustrated. However, physicians squander education opportunities if they prematurely abandon efforts to influence legislators after insufficient or no response to queries. When the effort is abandoned, victory is conceded to the opposition.
Do not burn bridges. Do legislators change their minds? The answer is an emphatic "yes." Most legislators are remarkably open-minded. With the exceptions of certain controversial emotional issues (eg, abortion, death penalty, gun control), those who persist often persuade legislators to take other viewpoints. Remember that most legislators are in office for years. Educating them can take time, but it is worth the effort.
Register to vote and exercise this right
Registered voters are the most influential citizens. The 2000 presidential election, which hung on the ballots of a handful of voters in Florida, testifies to the potential importance of even a small number of voters. Even under ordinary circumstances, the number of votes needed to swing an election can be small.
The author (a Democrat) serves as legislator in a district of Maryland that has 90,000 eligible voters out of an overall population of 120,000. Of these 90,000, approximately 50,000 are registered. Of these, 28,000 are Democrats and 22,000 are Republicans. In a primary election, voter turnout is typically less than 50%, often much less. Thus, 14,000 Democrats and 11,000 Republicans may go to the polls in a primary election. Lists that indicate which citizens voted in the last 3 primary elections are available; such citizens are considered prime voters. These prime voters typically show up to vote regardless of circumstances (eg, blizzard, broken leg). Approximately 8000 prime Democratic voters reside in the author's relatively affluent middle-class district.
In a district primary race in the Maryland State Legislature, the number of votes required to win election also depends on the number of candidates. In the preceding example, roughly 6000 votes would win the primary election. Thus, what started as a daunting task (to become elected in the state of Maryland) simply became a challenge to find 6000 voters to support the candidate. Of course, after the primary, one has to win the general election, but winning the primary is obviously an essential first step.
The smaller the number of votes that can affect the outcome of an election, the more each single vote counts. Elected officials have immediate access to voter rolls, and staff members know if someone contacting the office is registered. Certainly, legislators respond to those who are not registered, but politicians pay closer attention to registered voters, who have direct influence over their political futures. If citizens are not registered voters, they are not players in the game.
Identify up-and-comers
No elected official begins as an incumbent. Almost all had to work hard to win an election, and most started at lower offices. Most governors and senators—with the notable exceptions of those with notoriety in other fields—began serving the public on city councils, state legislatures, or other lower offices.
Developing influence with elected officials in higher offices and establishing and maintaining relationships with politicians who are getting started in politics and who appear likely to be successful, especially if views agree, is important. Newly elected officials are usually highly accessible and truly appreciate input from their constituents. As elected officials climb the political ladder, the influence of long-time supporters grows.
Contribute money and help campaign
This must be stated plainly: Running a campaign costs money. Citizens who contribute to a campaign are well regarded. This does not mean that politicians are owned or that a timely contribution buys a vote; most politicians are honest and ethical. Nonetheless, politicians appreciate citizens who understand the importance of financial donations to a successful campaign.
Appropriate, timely, and legal campaign contributions are part of the real-world price that must be paid to participate fully in the political process. Until campaigns are financed differently, any group that wishes to increase its ability to influence legislation must have a budget for political donations.
Candidates appreciate and remember those who help with other parts of the campaign, such as placing lawn signs, joining the candidate door-to-door or in parades, arranging neighborhood meetings, or working the polls on election day.
Share ideas
Politicians are not omniscient. A surprising number of pieces of important legislation originate with a constituent's letter or phone call.
If the legislator likes a submitted idea, the constituent need not be concerned about drafting the bill. The constituent physician can help by providing an outline of the key points, but each legislature provides lawyers who specialize in bill drafting so that bills are in proper legislative form.
The ED physician has a unique insight into almost every major social problem society faces, from environmental degradation to adolescent pregnancy to street violence to cardiac disease. Emergency physicians are on the front lines and provide care for all kinds of people. The thoughts and insights of emergency physicians will be taken seriously if seriously communicated to elected officials.
Although politicians expect input from citizens regarding personal economic issues, be sure to balance this by providing input regarding issues that are purely for social good (eg, toughening drunk-driving laws, promoting seat-belt use).
When lobbying on issues that affect personal financial well-being, remember that legislators earn less than physicians. The author once observed a prominent surgeon complain to a legislative committee that fee cutbacks would jeopardize his second home. Although committee legislators did not demonstrate emotion during the hearing, the comments in the back room afterward were devastating.
Build relationships
During the legislative session, most legislators are swamped from dawn to dusk. Their ability to hear new ideas and to process new concepts during this time is limited. The time to get to know an elected official is when the legislature is out of session.
Try to learn what the legislator likes to do. Do not be afraid to offer a low-key social invitation or to invite the legislator to address a community group, professional club, or just some friends gathered in the living room. Most politicians love an audience and the chance to meet new people.
If possible, invite a legislator to join you for an ED shift. Seeing what emergency physicians really do from their perspective is often a real eye-opener and a valuable experience for legislators.
Partnerships of interest groups especially carry weight when they come together on an issue. Building coalitions with other professionals (eg, nurses, paramedics, physician assistants, organizations, public interest groups) can establish key relationships.
Communicate effectively and appropriately
As 1 of 188 legislators in a state with a population of fewer than 6 million people, this author still receives as many as 40 pieces of mail daily when the legislature is out of session and as many as 150 communications daily when the legislature is in session. Write a single-page letter whenever possible. State your problem clearly and simply, preferably with a personal angle, and include ideas for solutions. If comprehensive in-depth material is required, include an executive summary.
Real letters from real people are always read. Mass mailings are noted but are less effective. Sending a newspaper article and adding a brief comment is sometimes a useful technique. Persistence pays: Continue making contact with short but frequent communications. Most politicians return calls from registered voters in their district. Do not assume legislators know medical jargon and abbreviations. To legislators in Maryland, for example, "DNR" means Department of Natural Resources rather than "do not resuscitate."
Support politicians of your choice
When in agreement with your legislator on an issue, communicate that agreement. When politicians feel that the public is supportive, they are more likely to promote specific positions and to work to influence other politicians. If legislators are unsure of public support, they may vote the citizen's way, but they do not push the issue as enthusiastically.
Letting politicians know when they do something that is appreciated is also important. Being a politician has its rewards, but it is not an easy job. Elected officials are often subject to personal attack from those who disagree with a position. More can be gained by forging a positive relationship than by creating a negative one; when an elected official does something right, send a letter of support. Like everyone, politicians appreciate praise. Just like emergency physicians, they often hear complaints, but hearing positive feedback for the good things is unusual and is highly appreciated.
Visit government in action
Most citizens are surprised to learn the degree to which their government is accessible. In Annapolis, the capital city of Maryland, citizens stroll the halls and pack hearing rooms. Testimony sign-up sheets are outside hearing rooms each day. The citizen does not have to be a lobbyist to participate: anyone can sign up to be heard on any issue.
Virtually every state has access to government on the Web. Familiarize yourself with your state government's Web site.
Most legislators, given reasonable notice, give visitors an insider's tour. An old saying states that "the two things one never should watch being made are sausage and the law," but a day spent in a state capitol actually provides great insight into the political process and into how a citizen can make a difference.
Democracy is a fragile thing, and many have given their lives for its existence. Government suffers when it lacks citizen participation. Most physicians are fortunate to have good jobs, good incomes, and personal stability. Physicians hold a unique place in the life of the community and a unique perspective on the needs of all those for whom they provide care. With that perspective comes an obligation to work to improve society. Active engagement with government is part of the way that obligation can be met. Being political can be seen as a natural extension of being an emergency medicine physician.
-
Here's one for ya nate:: http://www.heroinhelper.com
-
I wonder if there is a "crack head" forum some where on the net that is crying about how junkies on TV don't shoot up the correct way.

I bet there is...just their spelling and vocabulary....well..nevermind...
-
-
-
Some how I suspect that when 'systemlord,' figured out we weren't a bunch of wanna be push over whackers who would be echoing his cries of 'YEAH... NURSES SUCK DUDE!!' He has gone away never to be heard from again..!!!
ACE
-
I've got a great new upgrade to a product that we use every day inthe field but don't want to mention it unless someone here has the venture capital that could fund the product development and introduction to market. I think it will make our lives in the field, the ER's lifes easier and the patient comfort better.
If you have the venture capital to help me move this to market then we should talk. Please don't contact me just to find out what the product is just so you can bring it to market because I'm working on getting a patent on it.
M
What kind of capital are we talking about "Ruff," ballpark?
-
For those who are interested here's alittle more information on 'Dopamine'
Dopamine is an endogenous catecholamine that is the precursor to norepinephrine in the catecholamine synthetic pathway. When administered therapeutically, dopamine is a complex agent. Dopamine, through its direct effects, is a weak partial beta-agonist. When initially administered, it releases norepinephrine through a tyramine-like effect.[135] It is a potent (relative to its receptor affinities) neuronal uptake inhibitor and by direct action acts as an agonist at dopamine D1 postsynaptic vasodilator receptors[136] and D2 presynaptic receptors on blood vessels and in the kidney.[137] The affinities for beta1 , beta2 , and alpha1B receptors are shown in Table 23-5 , where it can be seen that dopamine has extremely low affinity for all three adrenergic receptors.At lower doses (≤2 µg/kg/min), dopamine causes a relatively selective dilation of splanchnic and renal arterial beds. This effect may be useful in promoting renal blood flow and maintaining GFR in selected patients who become refractory to diuretics, especially when caused by marginal renal perfusion. Dopamine also has direct renal tubular effects that promote natriuresis. At intermediate (2 to 10 µg/kg/min) infusion rates, dopamine, by virtue of its tyramine and neuronal uptake-inhibiting properties, enhances norepinephrine release from vascular and myocardial adrenergic neurons, thereby resulting in increased cardiac beta-adrenergic receptor activation and an increase in peripheral vascular resistance. In patients with advanced HF, who often have depleted intracardiac norepinephrine stores, dopamine is a less effective positive inotropic drug than are other "directly" acting inotropes. [128] [129] At higher infusion rates (5 to 20 µg/kg/min), peripheral vasoconstriction occurs as a result of direct alpha-adrenergic receptor stimulation. Increases in systemic vascular resistance are common even at intermediate infusion rates. On initial administration, tachycardia and arrhythmia tend to be more pronounced than with dobutamine[128] and are related to cardiac norepinephrine release.[135] [138]
In patients with advanced, decompensated HF, dopamine should not be used as a positive inotropic agent but rather should be used in low doses for renal perfusion and in intermediate to high doses to increase peripheral resistance. The latter property is often necessary for a variety of reasons, including sepsis, iatrogenic overvasodilation, and brain injury.
TABLE 23-5 -- Pharmacological Characteristics of Various Adrenergic Agonists Used to Treat Decompensated Heart Failure Agent Beta1 -Receptor Affinity (Kd , nM) Beta2 -Receptor Affinity (Kd , nM) Alpha1 -Receptor Affinity (Kd , nM) Uptake1 Affinity (nM) Intrinsic Activity * for Human Beta1 Receptors
Dobutamine 470 570 130 190,330 0.5
Dopamine 25,000 100,000 36,000 130,230 0.2
Epinephrine 20 20 160 1,400 1.0
Isoproterenol 20 20 >10,000 9,000 1.0
Norepinephrine 20 400 200 500,670 1.0
Phenylephrine >10,000 >10,000 1,000 >10,000 0
Median inhibitory concentration (IC50 ) data were converted to affinity constants using the Cheng-Prusoff equation.
Some data from Iverson LL (ed): The Uptake and Storage of Noradrenaline in Sympathetic Nerves. Cambridge, UK, Cambridge University Press, 1967.
*Relative to isoproterenol = 1.0 in nonfailing isolated human RV trabeculae. Affinity data are based on radioligand-cold ligand competition curves in (1) human ventricular myocardial membrane preparations (beta1 , beta2 , alpha1 in nonfailing hearts, norepinephrine, epinephrine, isoproterenol), (2) human recombinant beta2 receptors in COS cell membranes (isoproterenol, norepinephrine, and epinephrine), (3) DTT1 cell membranes (beta2 , dobutamine, and dopamine), and rat heart membranes (alpha1 , dobutamine). Additional alpha1 -agonist affinity data are derived from irreversible dibenamine antagonism in rabbit aorta, with
Management of Episodes of Acute Decompensation
As discussed earlier, acute manifestations of HF can either be in the context of new onset or be in subjects with established chronic HF. Treatment of acute episodes of HF are similar in these two scenarios, with the exception that a diagnostic work-up potentially leading to definitive therapy should be done in new cases. Since multiple-treatment modalities may be brought to bear on acute HF episodes, the discussion is
TABLE 24-4 -- Pharmacological Therapy for Acute, Decompensated Heart Failure Treatment Modality Specific Examples
Intravenous diuretics Furosemide, bumetatide, torsemide
Intravenous positive inotropic agents Dobutamine, milrinone, enoximone
Intravenous vasodilators Nitroprusside, nitroglycerine, nesiritide
Blood pressure, renal perfusion support Intravenous dopamine, intravenous vasopressin
divided into pharmacological and nonpharmacological forms of therapy.
PHARMACOLOGICAL THERAPY (see Chap. 23 ).
Table 24-4 gives the standard treatment modalities typically used to treat acute episodes of HF with advanced, Class IV symptoms. In general, treatment begins with intravenous diuretics, which in subjects with adequate organ perfusion often suffice to produce diuresis accompanied by a prompt drop in preload and relief of symptoms related to pulmonary edema. If peripheral perfusion is compromised or diuresis does not ensure, intravenous dobutamine, an inotropic beta/alpha-adrenergic agonist that produces an increase in cardiac output without substantially dropping preload or blood pressure, [129] or nesiritide (BNP)[130] (see Fig. 23-5 ), a vasodilator, can be added via a well-secured peripheral line. A PDEI such as milrinone[131] [132] or enoximone[133] [134] can also be used to treat decompensated HF but should not be administered without pulmonary artery pressure monitoring unless it is certain that left ventricular filling pressure is high (>15 mm Hg). The reason for this precaution is that PDEIs are such potent venodilators that in patients with normal or low filling pressure, they can drop preload to undesirably low levels. Finally, in decompensated subjects who are still receiving beta-blocking agents, a PDEI rather than a beta blocker is the treatment of choice because PDEIs retain full or even have enhanced activity in the presence of beta blockade.[135]
If the situation has not stabilized, additional inotropic support with or without supplemental afterload reduction is indicated and best delivered with the aid of pulmonary artery catheter monitoring. The combination of dobutamine and a PDEI is additive for effects on cardiac output and, via the PDEI, will produce a reduction in pulmonary artery and left ventricular filling pressure.[136] [137] The latter may provide welcome unloading of the right ventricle inasmuch as high pulmonary artery pressure can produce limiting right ventricular dysfunction in some patients.
Once optimal inotropic therapy is being delivered, pure vasodilators can be additionally administered to subjects with persistently high systemic or pulmonary vascular resistance. Vasodilators such as nitroprusside or nitroglycerin can also be used in lieu of a positive inotropic agent, particularly in patients with higher systemic vascular resistance. As a vasodilator, nesiritide has the unique property of preferentially increasing renal blood flow[138] [139] and theoretically may be of value in patients with compromised renal function; however, nesiritide may also precipitate renal failure and must be used cautiously in this setting.
Finally, in patients with blood pressure so low that renal perfusion is compromised, dopamine may be added to increase perfusion pressure and renal blood flow via this agent's alpha-adrenergic and dopaminergic properties. However, dopamine should not be considered an effective positive inotropic agent because the majority of its weak, partial beta-agonist effect is mediated by norepinephrine
TABLE 24-5 -- Nonpharmacological Therapy for Acute, Decompensated Heart Failure Treatment Modality Specific Examples
Oxygenation Supplemental oxygen, mechanical ventilation
Balloon counterpulsation Intraaortic balloon pump
VAD Pulsatile-flow LVAD
Pacing AV sequential pacemaker; biventricular pacing
Urgent cardiac catheterization PTCA, mitral valvuloplasty, pericardiocentesis
Urgent cardiac surgery CABG, AVR, MV repair or replacement, transplantation
AV = atrioventricular; AVR = aortic valve replacement; CABG = coronary artery bypass grafting; LVAD = left ventricular assist device; MV = mitral valve; PTCA = percutaneous transluminal coronary angioplasty; VAD = ventricular assist device.
release,[140] which results in tachyphylaxis within 12 hours of administration.
Adrenergic Agonists
Mechanism of Action
The most powerful way to increase contractility in the human heart is by the use of a beta-adrenergic receptor agonist. Beta-agonists operate through the mechanism that regulates contractility and heart rate on a beat-to-beat basis in the intact heart (see also Chap. 19 ).[110] As depicted in Figure 23-6 , this system is composed of two cell surface membrane receptors (beta1 and beta2 ); two G proteins (the stimulatory G protein, Gαs , and the inhibitory G protein, Gαi ); the adenylyl cyclase enzyme (which converts Mg-ATP to cAMP); cAMP-activated protein kinase (protein kinase A); compartmentalized phosphodiesterases, which modulate cAMP levels to produce selective signaling; and target structures whose phosphorylation leads to a positive inotropic effect by changes in Ca2+ handling (phospholamban, the ryanodine release channel, and slow inward current calcium channels). An important point in the function of beta-adrenergic pathways is that they are not all cAMP dependent[110] ; in Figure 23-6 the beta1 receptor is depicted with direct activation of voltage-sensitive Ca2+ channels as well as cAMP-dependent activation. The end result is a powerful positive inotropic as well as positive chronotropic effect.
In the failing human heart, beta-adrenergic pathways undergo desensitization, a pharmacological term encompassing the regulatory changes that occur in receptors, G proteins, and adenylyl cyclase.[111] [112] In advanced HF, the degree of beta-adrenergic receptor desensitization approaches 50 to 60 percent of the maximum capacity of signal transduction,[113] [114] and in severe HF, beta-agonists may no longer be able to support myocardial function.[115] However, the vast majority of patients with advanced HF still exhibit a substantial inotropic response to beta-agonists,[114] which is the basis for their usefulness as inotropic agents in the treatment of decompensated HF.
All beta-agonists are given intravenously for short-term support of decompensated HF. They are all arrhythmogenic to some extent through direct mechanisms as well as through increasing the skeletal muscle deposition of potassium[40] and important consideration in the heart, which has the most active uptake1 system of any organ and uses neuronal reuptake to terminate the majority of the action of released norepinephrine.
Although beta1 - and beta2 -adrenergic receptors are coupled to positive inotropic and chronotropic responses through cAMP-dependent and -independent mechanisms, these two receptors have important differences. For one thing, beta1 receptors are positioned inside or near the synaptic cleft area to mediate the effects of released norepinephrine, which also means that catecholamines that have high affinity for neuronal reuptake do not reach myocardial beta1 receptors unless neuronal reuptake is functionally decreased (as it is in myocardial failure) or absent (as it is in a recently [<2 years] transplanted heart). In addition, a growing body of evidence indicates that chronic beta1 receptor agonist occupancy or pathway activation, or both, is more deleterious than beta2 receptor activation.[110] [118] However, from an acute support standpoint, both receptors can be used in supporting cardiac function in decompensated patients.
NEURONAL REUPTAKE AFFINITIES FOR SYMPATHOMIMETIC AMINES.
Table 23-5 lists the adrenergic receptor and neuronal reuptake (uptake1 ) affinities for catecholamines that are used therapeutically to increase cardiac performance or increase systemic vascular resistance or blood pressure. Although the primary action of uptake1 is to terminate the action of norepinephrine, the functional status of uptake1 is also an important determinant of catecholamine therapeutic action when these agents are administered exogenously. For example, epinephrine, which has an affinity for uptake1 that is slightly lower than that of norepinephrine, is a much more potent therapeutic catecholamine when administered to denervated cardiac transplant hearts than to innervated hearts. [119] [120] When the heart is innervated, uptake1 removes much of the systemically administered epinephrine before it can reach myocardial beta1 -adrenergic receptors, which are preferentially located within the synaptic cleft area. In contrast, isoproterenol, which has essentially no affinity for uptake1 , is equally effective in innervated and denervated hearts.[121] [122]
The failing human heart has a functional impairment in uptake1 that essentially creates functional denervation, which in the case of catecholamines with higher affinity for uptake1 can offset some of the postsynaptic desensitization changes. Another way in which uptake1 can influence drug action is to compete with neurotransmitter norepinephrine for neuronal reuptake, which increases the amount of norepinephrine available in the synaptic cleft area. As can be observed in Table 23-5 , the substituted synthetic catecholamine, dobutamine, and the endogenous catecholamine, dopamine, have even higher affinity for uptake1 than does norepinephrine, and at least in the case of dopamine, this higher affinity contributes to its predominant inotropic action, which is to potentiate norepinephrine release.
BETA-ADRENOCEPTOR AGONISTS.
When left ventricular failure is severe, as manifested by marked reduction of cardiac index (<2 liters/min/m2 ), and pulmonary capillarywedge pressure is at optimal (18–24 mm Hg) or excessive (>24 mm Hg) levels despite therapy with diuretics, beta-adrenoceptor agonists are indicated. Although isoproterenol is a potent cardiac stimulant and improves ventricular performance, it should be avoided in STEMI patients. It also causes tachycardia and augments myocardial oxygen consumption and lactate production; in addition, it reduces coronary perfusion pressure by causing systemic vasodilation and in animal experiments it increases the extent of experimentally induced infarction. Norepinephrine also increases myocardial oxygen consumption because of its peripheral vasoconstrictor as well as positive inotropic actions.
Dopamine and dobutamine (see Chap. 23 ) can be particularly useful in patients with STEMI and reduced cardiac output, increased left ventricular filling pressure, pulmonary vascular congestion, and hypotension. Fortunately, the potentially deleterious alpha-adrenergic vasoconstrictor effects exerted by dopamine occur only at higher doses than those required to increase contractility. The vasodilating actions of dopamine on renal and splanchnic vessels and its positive inotropic effects generally improve hemodynamics and renal function. In patients with STEMI and severe left ventricular failure, this drug should be administered at a dose of 3 µg/kg/min while pulmonary capillary wedge and systemic arterial pressures as well as cardiac output are monitored. The dose can be increased stepwise to 20 µg/kg/min to reduce pulmonary capillary wedge pressure to approximately 20 mm Hg and elevate cardiac index to exceed 2 liters/min/m2 . It must be recognized, however, that doses exceeding 5 µg/kg/min activate peripheral alpha receptors and cause vasoconstriction.
Dobutamine has a positive inotropic action comparable to that of dopamine but a slightly less positive chronotropic effect and less vasoconstrictor activity. In patients with STEMI, dobutamine improves left ventricular performance without augmenting enzymatically estimated infarct size. It can be administered in a starting dose of 2.5 µg/kg/min and increased stepwise to a maximum of 30 µg/kg/min. Both dopamine and dobutamine must be given carefully and with constant monitoring of the electrocardiogram, systemic arterial pressure, and pulmonary artery or pulmonary artery occlusive pressure and, if possible, with frequent measurements of cardiac output. The dose must be reduced if the heart rate exceeds 100 to 110 beats/min, if supraventricular or ventricular tachyarrhythmias are precipitated, or if ST segment changes increase.
Nitroglycerin.
This drug has been shown in animal experiments to be less likely than nitroprusside to produce a "coronary steal"—that is, to divert blood flow from the ischemic to the nonischemic zone. Therefore, apart from consideration of its routine use in STEMI patients discussed earlier, it may be a particularly useful vasodilator in patients with STEMI complicated by left ventricular failure. Ten to 15 mg/min is infused and the dose is increased by 10 mg/min every 5 minutes until (1) the desired effect (improvement of hemodynamics or relief of ischemic chest pain) is achieved or (2) a decline in systolic arterial pressure to 90 mm Hg, or by more than 15 mm Hg, has occurred. Although both nitroglycerin and nitroprusside lower systemic arterial pressure, systemic vascular resistance, and the heart rate-systolic blood pressure product, the reduction of left ventricular filling pressure is more prominent with nitroglycerin because of its relatively greater effect than nitroprusside on venous capacitance vessels. Nevertheless, in patients with severe left ventricular failure, cardiac output often increases despite the reduction in left ventricular filling pressure produced by nitroglycerin.
Cardiogenic Shock
Cardiogenic shock is the most severe clinical expression of left ventricular failure and is associated with extensive damage to the left ventricular myocardium in more than 80 percent of STEMI patients in whom it occurs; the remainder have a mechanical defect such as ventricular septal or papillary muscle rupture or predominant right ventricular infarction.[27] In the past, cardiogenic shock has been reported to occur in up to 20 percent of patients with STEMI, but estimates from recent large randomized trials of fibrinolytic therapy and observational databases report an incidence rate in the range of 7 percent.[27] About 10 percent of patients with cardiogenic shock present with this condition at the time of admission, whereas 90 percent develop it during hospitalization. This low-output state is characterized by elevated ventricular filling pressures, low cardiac output, systemic hypotension, and evidence of vital organ hypoperfusion (e.g., clouded sensorium, cool extremities, oliguria, acidosis). Patients with cardiogenic shock due to STEMI are more likely to be older, to have a history of a prior myocardial infarction or congestive heart failure, and to have sustained an anterior infarction at the time of development of shock. Of note, although the incidence of cardiogenic shock in patients with STEMI has been relatively stable since the mid-1970s, the short-term mortality rate has decreased from 70 to 80 percent in the 1970s to 50 to 60 percent in the 1990s.[183] Cardiogenic shock is the cause of death in about 60 percent of patients dying after fibrinolysis for STEMI.
Medical Management
When the aforementioned mechanical complications are not present, cardiogenic shock is due to impairment of left ventricular function. Although dopamine or dobutamine usually improves the hemodynamics in these patients, unfortunately neither appears to improve hospital survival significantly. Similarly, vasodilators have been used in an effort to elevate cardiac output and to reduce left ventricular filling pressure. However, by lowering the already markedly reduced coronary perfusion pressure, myocardial perfusion can be compromised further, accelerating the vicious circle illustrated in Figure 46-10 . Vasodilators may nonetheless be used in conjunction with intraaortic balloon counterpulsation and inotropic agents in an effort to increase cardiac output while sustaining or elevating coronary perfusion pressure.
The systemic vascular resistance is usually elevated in patients with cardiogenic shock, but occasionally resistance is normal and in a few cases vasodilation actually predominates.[186] When systemic vascular resistance is not elevated (i.e., <1800 dynes/sec/cm5 ) in patients with cardiogenic shock, norepinephrine, which has both alpha- and beta-adrenoceptor agonist properties (in doses ranging from 2 to 10 µg/min), can be employed to increase diastolic arterial pressure, maintain coronary perfusion, and improve contractility. Norepinephrine should be used only when other means, including balloon counterpulsation, fail to maintain arterial diastolic pressure above 50 to 60 mm Hg in a previously normotensive patient. The use of alpha-adrenoceptor agents such as phenylephrine and methoxamine is contraindicated in patients with cardiogenic shock (unless systemic vascular resistance is inordinately low). Inspired by the observation that many patients with shock have a low systemic vascular resistance, Cotter and associates evaluated the benefit of the nitric oxide synthase inhibitor L-NMMA in patients in refractory shock.[187] The favorable impact of L-NMMA on the hemodynamics and clinical outcomes in this pilot study serves as the foundation for further investigation of nitric oxide synthase inhibition of cardiogenic shock.
-
I'm interested in the requirements of UK EMS where can I find more information on it?
Above here, by doing a search at EMTCITY for international ems, and at www.international-ems.com....
OUt Here,
ACE844
-
excelent, what search engine do you use?
 LighteningFastACE search.com
LighteningFastACE search.com 
Actually you just happened to catch me studying using "Zipes: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 7th ed., Copyright © 2005"
ACE844
-
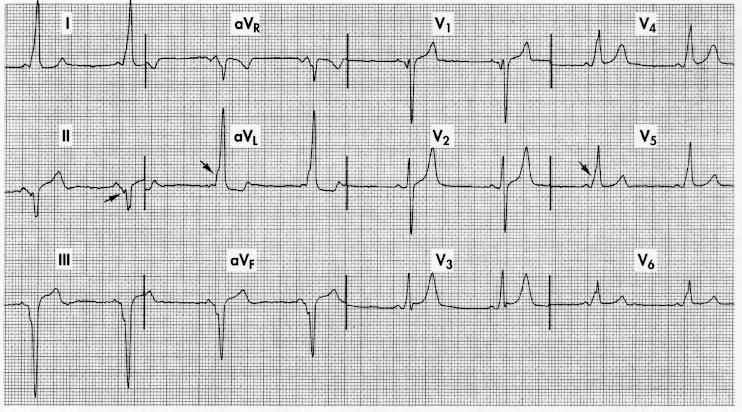
Here's your 12-lead you requested
http://www.ecglibrary.com/wpwaf.html
http://www.ecglibrary.com/wpwaf2.html
http://en.wikipedia.org/wiki/Wolff-Parkinson-White_syndrome
http://www.clevelandclinic.org/heartcenter...mp;thirdCat=259
Treatment of AFib associated with WPW is necessarily different than for a patient with a normal heart. AFib is an irregular rhythm as opposed to the regular rhythm seen in CMTs.The basic treatment principle in WPW AFib is to prolong the anterograde refractory period of the accessory pathway relative to the AV node. This slows the rate of impulse transmission through the accessory pathway and, thus, the ventricular rate. This is in direct contradistinction to the goal of treatment of non-WPW AFib, which is to slow the refractory period of the AVN.
If AFib were treated in the conventional manner by drugs that prolong the refractory period of the AV node (eg, calcium channel blockers, beta-blockers, digoxin), the rate of transmission through the accessory pathway likely would increase, with a corresponding increase in ventricular rate. This could have disastrous consequences, possibly causing the arrhythmia to deteriorate into V fib.
Thus, standard treatments for non-WPW AFib must be avoided and replaced by cardioversion with the possibility of procainamide as a potential medical therapeutic alternative. Patients presenting with Afib in WPW syndrome are typically very tachycardic and often hypotensive with evidence of hypoperfusion, thus given this unstable state, primary synchronized cardioversion should be the first-line treatment.
If the patient is stable, medical therapy with procainamide may be tried. Procainamide (17 mg/kg IV infusion, not to exceed 50 mg/min; hold for hypotension or 50% QRS widening) blocks the accessory pathway, but it has the added effect of increasing transmission through the AV node. Thus, although procainamide may control the AFib rate through the accessory pathway, it may create a potentially dangerous conventional AFib that may require treatment with other medications and/or cardioversion. Prompt cardioversion of patients with WPW syndrome and AFib may be required for any patient who is deteriorating or failing to improve.
Medical management may be a viable option in some patients, but it may have unpredictable results. Note that cardioversion is always the treatment of choice in unstable patients. If medical management is recommended it should be under the direction of a cardiologist.
Treatment of CMTs (regular and generally narrow complex tachycardias) associated with WPW syndrome yields several treatment approaches. Unfortunately, there is a paucity of literature and controlled studies, which makes the chosen treatment less definitively advocated. The two common approaches include cardioversion and the use of adenosine. If adenosine is chosen, all preparations for immediate cardioversion and appropriate resuscitation should be in order in the event of degeneration of the rhythm after adenosine-induced AV nodal blockade
In a stable patient with a regular narrow complex tachycardia (not known to be a result of WPW syndrome), adenosine (6 mg rapid IV push; if unsuccessful, 12 mg rapid IV push) should be the first-line treatment. (Adenosine is contraindicated in heart transplant patients and should be used with caution in patients with severe obstructive pulmonary disease and in patients with a wide QRS complex, unless the diagnosis of PSVT with aberrancy is certain.) When WPW syndrome is known or highly likely, adenosine should be used with caution and preparation for cardioversion/defibrillation should be immediately available.
Once the circus movement is broken, the patient usually converts to sinus rhythm. Note that whether the QRS complex is regular or irregular distinguishes CMTs from AFib on ECG.
If the QRS complex is regular and narrow, the arrhythmia may be treated with adenosine as if it were CMT or PSVT, as long as preparations for cardioversion/defibrillation are immediately available.
If the QRS complex is irregular, the arrhythmia is likely AFib. In this case, adenosine theoretically could increase the rate and cause clinical deterioration and should not be used.
Cardioversion, or in some cases, procainamide, are the treatment choices in these situations (ie, irregular QRS complex), providing the necessary rate control.
If in doubt about the regularity of the rhythm, it is safer to err on the side of treating for AFib in the context of WPW syndrome with direct cardioversion.
(Goldberger: Clinical Electrocardiography: A Simplified Approach @ 6th ed.,)
Wolff-Parkinson-White PatternThe WPW syndrome is an unusual and distinctive ECG abnormality caused by preexcitation of the ventricles. Normally the electrical stimulus passes to the ventricles from the atria via the AV junction. The physiologic lag of conduction through the AV junction results in the normal PR interval of 0.12 to 0.2 second. Imagine the consequences of having an extra pathway between the atria and ventricles that would bypass the AV junction and preexcite the ventricles. This is exactly what occurs with the WPW syndrome: an atrioventricular bypass tract * connects the atria and ventricles, circumventing the AV junction (Fig. 10.18) .
Preexcitation of the ventricles with the WPW syndrome produces the following three characteristic changes on the ECG (Figs. 10-19 and 10-20) :
The QRS is widened, giving the superficial appearance of a bundle branch block pattern. However, the wide QRS is caused not by a
--------------------------------------------------------------------------------
* Formerly called the bundle of Kent.
--------------------------------------------------------------------------------
delay in ventricular depolarization but by early stimulation of the ventricles. (The QRS is widened to the degree that the PR is shortened.)
The PR is shortened (often but not always to less than 0.12 second) because of ventricular preexcitation.
The upstroke of the QRS complex is slurred or notched. This is called a delta wave.
Figs. 10.19 and 10.20 show the WPW pattern, with its classic triad of a widened QRS, a short PR interval, and a delta wave. Notice that the pattern superficially resembles a bundle branch block pattern because of the widened QRS complexes. Depending on which area of the ventricles is preexcited first, the ECG may show a pattern simulating that of either RBBB with tall R waves in the right chest leads or LBBB with a predominantly negative QS in lead V1 .
The significance of WPW preexcitation is twofold:
Patients with this pattern are prone to arrhythmias, especially paroxysmal supraventricular tachycardia (PSVT) (Fig. 10.21) .
The ECG of these patients is often mistaken as indicating a bundle branch block or MI (see Fig. 10.20) .
The WPW syndrome predisposes patients to develop paroxysmal supraventricular tachycardia (PSVT) because of the presence of an extra conduction pathway. For example, a premature impulse
traveling down the AV junction may recycle up the accessory pathway and then back down the AV junction, and so on. * This type of recirculating impulse is an example of reentry.
Another type of preexcitation variant, the Lown-Ganong-Levine (LGL) syndrome, is caused by a bypass tract that connects the atria and AV junction. Bypassing the AV node results in a short PR interval (less than 0.12 second). However, the QRS width is not prolonged, because ventricular activation occurs normally. Therefore the LGL pattern consists of a normal-width QRS complex with a short PR interval and no delta wave; the WPW consists of a wide QRS complex with a short PR interval and a delta wave (see Fig. 10.19) .
Patients with the LGL pattern may also have reentrant-type PSVT or paroxysmal atrial fibrillation or flutter. *
And Here's 2 more images for ya.
Scenario
in Education and Training
Posted
OK, the short quick immediate answers are as follows...2+ large bore IV's, labs, 325 ASA PO {Barring contraindications} Low flow o2, as already started, a follow up 12-lead in a few minutes, and BENZO'S until anxiolysis-symptomtology reduction is achieved..extriacte to the ambulance and transport, as care is supportive mostly in this case.