


BEorP
-
Posts
840 -
Joined
-
Last visited
-
Days Won
9
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by BEorP
-
-
I also have a big problem with the resistance that we often seem to have to doing any assessment that won't directly impact how we care for the patient. In an unconscious, apneic patient from the rough side of town should I bother to look at the pupils or should I just bag them since that is what I'm going to do regardless? Should we not bother to do 12 lead for suspected cardiac ischemia patients in places without STEMI bypass since it will not directly change our treatment?
Not doing assessments because it won't directly affect something that we will be doing goes down a dangerous slippery slop to being anything but health professionals.
-
 2
2
-
-
the trauma center told me to go wherever I wanted and I could talk to patients. However I didn't have the direction I did at the other hospital. I don't know. Speaking to the my instructor , he had the same problem there during his clinicals and found a much better experience elsewhere. Some places just seem to be better teaching hospitals.
Although maybe not seeming as fun as being "hands on," do not underestimate the importance of practicing history taking, which you have a lot of freedom to do in this type of situation where no one is paying much attention to what you are doing. I agree that it is probably not ideal to not be under someone's wing, but if you're in that situation again I would suggest that you just go patient to patient (with patients who will tolerate being bothered by a student) and take a good history. Being able to take a good history in a reasonable amount of time does take practice even though asking a set of questions seems like it should be easy.
If you are left on your own to do whatever you want, you might as well also at least do some kind of assessment on the patients. Lung sounds is probably one of the most important assessment skills for a student prehospital provider to be able to assess well. Everyone has lungs so even if they aren't in with a respiratory problem, have a listen. Knowing normal will make it easier to recognize abnormal.
-
ContinuingEducation.com has some good ones. I particularly like that a lot of them focus more on knowledge in certain areas that may not directly impact your practice today but that we should all still know as health professionals.
(For full disclosure, I have done some work for them.)
-
A pocket mask would probably be a much better option for your purposes. Cheaper and easier to use.
-
For me, how death has occurred often determines how it impacts me. Occasionally we do see someone who had what I would consider a good death (e.g. long life, maintained independence until the end, died at home, had good health up until death, etc.). Though it is sad for the family having lost a loved one, it doesn't bother me after the call is over. What I find more difficult are some of the bad deaths we are involved in, especially when things could have so easily gone a better way (e.g. a hanging, needing to try to resuscitate someone who was known to be terminal and getting them back only to spend a couple of days in ICU, etc.).
I think we need to be careful when judging other people's reactions to death though. If Trm90 is simply sharing how he truly feels, I don't see a need to criticize. We all deal with the things we see in this job differently. Maybe someday he will look back and feel differently about his experiences. We would criticize someone who comes on here saying that they want to get into this industry because they "want to help people" so why do we also criticize someone who doesn't have strong emotions connected to the personal aspect of the job? As long as he is doing his job appropriately, including his communication with the family, it sounds to me like he may have a recipe for career longevity that will far exceed mine.
-
I'll include the caveat that this is just from my experience and is my opinion, but I don't think you need to worry too much about this thing about what looks good on a resume. If you have a BSc, your paramedic diploma, and have passed or will pass the AEMCA then you're probably in a good position. Often, the resume just really needs to get you to the written test in the recruitment process (obviously not all services will be the same, but this seems to be fairly common now). There isn't a whole lot of resume screening usually when there is a written test, so little things like patient transfer and lifeguarding probably won't matter. It is likely that everyone who has the basic qualifications will be invited to write the written test and if there is any screening, your degree should position you well.
Now, if "looks good on a resume" means more "is good experience to discuss in an interview", I guess I would give it a little bit more consideration. I would think more that the benefit would come from having experience to cite to answer the typical interview questions (Google them if you're not familiar with them), rather than saying "I worked patient transfer, I can work a stretcher" or "I was a lifeguard, I know CPR". This experience to call upon when answering interview questions could likely come from any work environment or just life experience in general.
I will just add as general advice to anyone who reads this thread that if you do patient transfer, event medical standby, lifeguarding, ski patrol, etc. you need to be careful how you discuss it in the interview. Far too many keen young paramedic applicants show up at job interviews talking about these experiences as if it means that they have essentially already been working as a paramedic. It may be applicable experience in some respects, but it isn't the same as being a paramedic so make sure it does not come across as you thinking that you're basically an experienced paramedic already when applying for your first job.
-
I would say that getting hired right now depends on a few main things:
- Connections made while riding out
- Knowledge and skills as assessed by the service on a written test or scenarios
- Ability to interview well
- Luck
Many services now use the Ability Works physical test that is fairly challenging and has unfortunately caused many people to lose out on job offers because of this. If there is any possibly that this will be an issue, get to the gym now.
Remember that there are far, far more AEMCAs than jobs each year in addition to the AEMCAs from previous years who have not been hired. The job situation does not seem to be getting any better. Be prepared for the possibility that you will graduate and not be able to find work and that if you are in the lucky few who do, it will be casual only.
I do not factor patient transfer experience in there at all. All paramedic graduates will know how to work a stretcher just as well as those who have done patient transfer. Some people will disagree with me and I may have a bias since I never worked patient transfer, but that is my opinion. Patient transfer isn't a bad part time job while you're in school, but I would not consider it an advantage in the hiring process for most services.
If heading to Alberta is a possibility for you, check which programs have CMA accreditation as this may make it easier. I don't know off the top of my head which programs have it now. I will add the important caveat that CMA accreditation is not a true marker of excellence in paramedic education but it can make it easier to move to another province (although it will still be possible if you attend a non-CMA accredited program).
-
Not really sure whether I can give any useful advice but I wanted to reply since I now see that you asked before for Ontario advice and got no replies. As you have read, Centennial and Humber are both well established and strong programs. I have worked with many Conestoga grads and it seems like a decent program as well. I wouldn't put Centennial down just because they have a bigger class size than Conestoga though. Have you been accepted to all three?
In terms of general advice, I would just say that you really need to be aware what you're getting yourself into in Ontario these days. If you can get a job, it will pay very well but will likely be part time casual for the first few years where you will work without a set schedule or partner, without benefits, without guaranteed hours, doing the shifts that others don't want to work (e.g. weekends, all summer). It may not sound that bad when your focus is just on getting to your goal of being a paramedic, but living it is becomes difficult to tolerate after a few years. Maybe others tolerate it better than me or I'm just tired and cranky though!
There is no real need for pre-reading or anything but if you want to read something then anatomy and physiology is always a good place to start. Once you're in school just keep up with the work and always ask "why?". Some people feel that part time work doing patient transfer is helpful on a resume, though I would tend to disagree and think that your ability to function as a paramedic (even if tested in a scenario) is much more important. Spend as much time doing scenarios in your paramedic lab as possible (especially if they have it open after hours). Not only may this time pay off in helping you to perform well on scenario testing to get a job, but it might also help you to make a decision that might actually matter to a patient's outcome sometime down the road. There's probably lots more that can be said, but those are the first tips that pop into my head.
Good luck!
-
I am a PA member. I do question a bit what I am actually getting for my money, but I am a member for two primary reasons:
1. In principle, I think that it is good to be a member of our professional organisation if we want to continue to advance (though I agree that with PA there is a high price to pay for this!)
2. More importantly for me, I have not worked ambulance in Australia but am applying for industrial paramedic jobs and I feel like having PA membership and completing the PA CPD program makes me look more like a real Australian paramedic to Australian employers
The conferences are also good, but you could attend these and just pay the non-member price so I can understand why people may not be interested in being PA members. Unfortunately, I have found the PA to not always be very responsive to my issues as a member but apparently they will be hiring someone to help with some administrative things to improve the situation.
So I guess in my specific situation, I think that being a member is worth it (though maybe just barely!), but I do understand why others might not feel as though it is worth it for them.
-
Thanks guys. We were recently issued new glucometers by our health region that included the reloadable pen device. I challenged them on the use of the devices because the standard of practice has prohibited their use for almost a decade. They haven't responded, but I refuse to use them.
Good call! They may want to look into what happened in this case: http://www.cbc.ca/news/canada/manitoba/story/2012/06/06/mb-diabetes-tests-southeast-collegiate.html
The specific details of the potential exposure aren't completely clear from the news article (it refers to a "diabetes testing pen"), but it does say:
"The device — the little pen-like device — is meant to be a single-user device. The device itself should not be shared between people," said Dr. Cheryl Rockman-Greenberg, head of the pediatrics and child health department at the university's medical school.
The lancets were changed for each person, Rockman-Greenberg said, but the professor did not realize the pen itself is not safe for use by multiple individuals.
-
Okay, so how did you deduce which province he's located in? I've read his posts over twice and looked through his profile and I still can't figure it out. That's why I never bothered responding.
I made a bad assumption (sorry!). I always associated numbered driver's licence classes with Alberta and BC but I now see that many other provinces have them and it is us in Ontario who is odd with our alphabetic system.
-
Thanks. I just wanna be sure about taking this profession and wanna know more what it's like when off the job. The required science courses I have done last sem but now I'm doing nothing but working on the other credentials like Class 4 Driver's Licencse, CPR or Basic Life Support I will take which is one class, and working on my body to be fit and pass the fitness test. I'm worried about making the wrong decision and find out a year later that this job is not for me because of issues in life.
Welcome to the forum. You're in a pretty good province to be considering a paramedicine career. In terms of what it is like off the job, I personally don't think that has much to do with anything when it comes to relationships. Yes, the shift work can be a burden and we do sometimes see things that might affect you psychologically but overall I do not see any reason why we would be more dysfunctional than other professions. The exception to this would be in Ontario where new PCPs often need to work PT casual for the first number of years, which involves a lot of last minute call ins that can become difficult for making any kind of social plans around. I don't think that this is the case out west, but hopefully one of our members there can chime in on what it is like for new employees in this respect.
So I guess what I am saying is that the job may or may not be for you, but if it isn't for you I don't think that it will be because of issues while off the job. Unlike American TV, most of us who do ambulance work in Canada do not eat, sleep, and breathe it. Home time is home time and we work a reasonable number of hours for a good wage so there are not the issues with having enough time off that our American friends sometimes encounter.
In Canada things are similar to other countries such as Australia, NZ and UK where Paramedic is an educated, well paid professional position.
I know the pay in BC, Alberta and Ontario is very good (PCP is about $25 an hour and ACP more) while I think the pay in NS is a bit less but still quite good, other provinces not so much from what I hear. The whole internal labour thing means that scope of practice will soon become standardised and national registration will be achieved from what I understand.
There are many Canadian Paramedics here and I don't know any of them who bitch and moan about being overworked, burnt out, underpaid etc or who upgrade to being a Nurse to get paid more, or who moan about being stuck 20 years behind the rest of the world in some respects of practice because their medical director is a douchebag.
I'd say go for it mate
I'll generally second what Kiwi has said here, but with a few minor modifications. In Ontario we are actually stuck more than 20 years behind the rest of the world in some respects because of all of our medical directors, but I don't moan and bitch about it too much since PCPs are paid around $35 an hour where I work (ACPs around $37). I'm not exactly sure on the pay out west, but it is still decent certainly and they are not as far behind the world as us in Ontario on things like PCP analgesia.
-
If you have 20 minutes to spare, you might find this NPR podcast interesting: http://www.npr.org/blogs/money/2012/12/18/167265874/episode-424-how-much-is-a-firefighter-worth
It is one of the first times I have heard any journalist-type actually understand that things don't burn like they used to...
-
What college are you at now? It is likely that it will be much easier to re-take there rather than applying all over again.
-
Hey guys,
The ACoP has not been so responsive, so I was just hoping someone might be able to confirm that I have understood things correctly. As an active Ontario PCP, do I understand correctly that I can get registered in AB with a restricted EMT-A license without needing to sit any exams in person?
Thanks!
-
Wow! Any idea what I could get for my ticket on the black market?
-
1
-
-
As others have said, it all depends on how you are evaluating the learning. If you gave the National Registry EMT-B test to a group who had just taken a 150 hour US EMT-B course and to a group a newly graduated degree paramedics from Australia, I would not be surprised if the better educated paramedics did no better.
I suspect that this would be the challenge in trying to research this type of thing as well. It will be difficult to come up with a truly valid test and two nearly identical groups to do the different courses. Even with that much working out, the applicability of the results to any setting other than where the study was conducted would probably be limited.
-
2
-
-
Thanks for all the replies! Glad I wasn't completely off base... still lots to learn though!
-
If you want to fly me out from Ontario for a weekend in Saskatchewan when you're short, I'll work for free if I get a tour around town as well! I'll sign up on your website so you've got my info just in case you want to take me up on that

It looks like a decent setup you've got there! One thing I was curious about though is the line that says, "Join North America’s #1 EMT Community." Since it is meant to be Canadian, is there a reason you chose to use EMT instead of paramedic there? I know the EMT terminology is still used by a couple of provincies, but I just like to see us embracing the professional title of paramedic so I had to ask.
-
It should get bigger if you click on it.
-
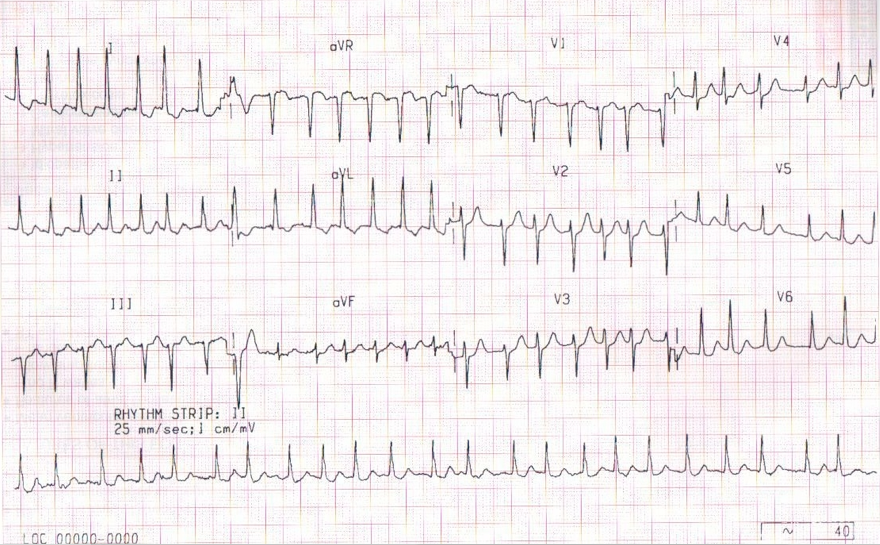
Hey guys, I'm just hoping to get some help with this ECG as I try to get better at reading these. Based on no clear P waves and it being slightly irregular, I want to call it AF. It is also tachy at around 180 though and with how it looks like any attempt at a P wave is often being buried in the T wave, it seems like that would make it more an SVT. Is it possible that this technically is both AF and an SVT? Any help is appreciated!
-
Most useless parameter in emergency medicine....

I would have to disagree. You might want to take a read of this: https://www.mja.com.au/journal/2008/188/11/respiratory-rate-neglected-vital-sign
-
Interesting thread. Just a question here for chbare or anyone who knows since we're talking CPAP and COPD. I had been under the impression that in COPD, the CPAP is basically counteracting the loss of radial traction and increased resistance (loss of positive transmural pressure) that has led to the bronchioles collapsing as the equal pressure point moves down below the cartilage supported airways.
Is there something going on with the alveoli specifically as well?
-
I've sorted things out and I will definitely be there for Day 2. Who is going to be joining me?
-
2
-
Clinicals!
in Education and Training
Posted
I guess the point that I was trying to make is more just that clinical placements often seem less than ideal but it will really end up being up to you to make the most of it. If there were a bunch of lower acuity patients that the nurse was assessing, you could have asked if you could go in and speak with them before the nurse did to take 5 minutes or so to get a history and then try presenting it to the nurse as if you brought the patient in and were giving a report. Or if that wouldn't work logistically (e.g. no place for you to speak with the patients), then you could have tried asking if you could ask some questions to get the history started even with the nurse right there.
I obviously wasn't there so I don't know exactly what would have worked in this situation, but there is almost always a way to make a bad clinical placement into something worthwhile. I am not trying to criticize you but I am trying to offer real suggestions for how you could make the most out of one in the future that may seem less than ideal since obviously you are quite ambitious and eager to learn.