


BEorP
-
Posts
840 -
Joined
-
Last visited
-
Days Won
9
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by BEorP
-
-
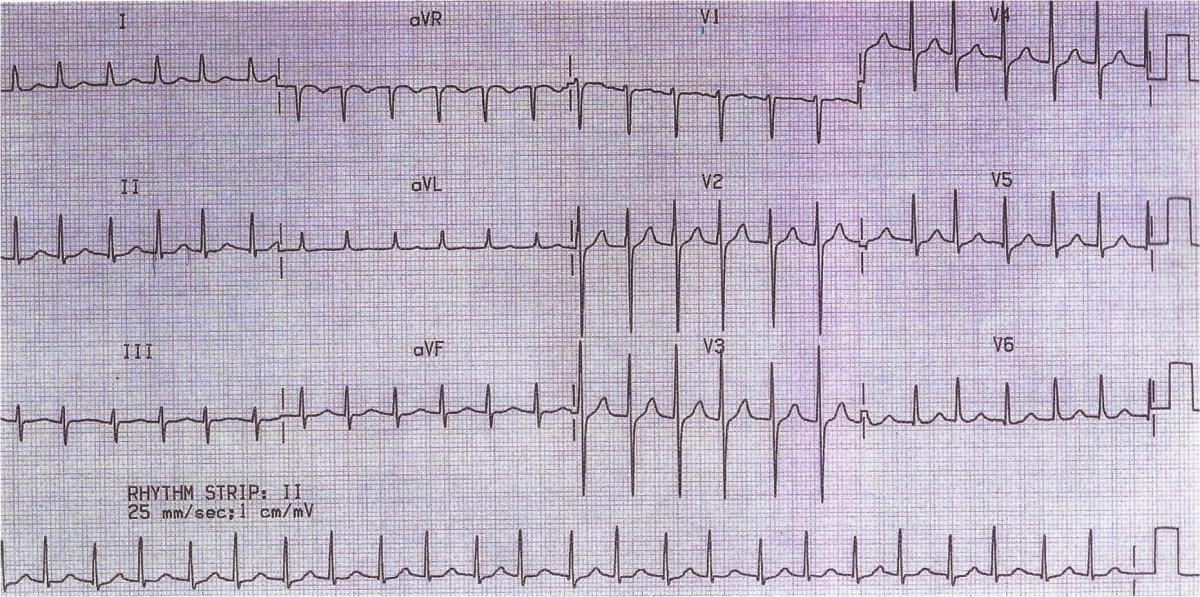
Just to give a little no-update-update, I haven't been able to come up with any reasoning for the variations in QRS amplitudes. It might end up going unexplained, but if I ever figure it out I will update the thread.
-
I don't have the full interpretation with me at the moment, but there was no mention of the possible electrical alternans and the overall interpretation was AF.
-
On the bottom lead (I assume lead II) view every other complex has the same R-wave height, almost like a slight electrical alternans.... Is this what you are referencing?
Yes, that is what I was most curious about. The irregularity in the rhythm is very minor, but very significant to the overall interpretation. The differing R-wave heights is obviously pretty minor compared to the example ECGs of electrical alternans floating around there (and clinically we wouldn't be expecting a spontaneous massive pericardial effusion in this patient), but I guess ultimately my question is when a finding like this becomes significant enough that it is worth reporting.
If I'm not just seeing things (which I'm not entirely convinced of yet), I guess the next logical question is whether we can speculate as to the possible mechanism in this case. From the little bit that I have read, it seems like there is debate over the causes of this in patients without pericardial effusion (but then again the ECG book recommended by ERDoc hasn't arrived yet so maybe I need to check there once it does).
-
This isn't an actual patient I saw but rather just a practice ECG. The clinical information is that it is a 66 year old female with palpitations. I'll share my thoughts on it later (since I've looked at the answer I don't want to spoil it... I'm interested in seeing if anyone saw what I thought I saw). The ECG should be attached.
Edit: looks like the attachment didn't work but at first but it should be attached now

-
Well, as i said, and thoiugh few will really admit, GCS is often estimated in the field instead of an emt going through the whole point-by-point asessment. If one is familiar with the GCS, and when time is of the essence and it has to be calculated stress, that's not a bad idea really to be able to estimate it.
I know that I am getting in late here, but I disagree with the whole premise of the question. Many "estimates" of GCS that I see done prehospitally get it completely wrong so I go through it properly. As others have pointed out, GCS may not be the best way to assess level of consciousness but if we are using it then we should use it correctly. All too often I see a patient being scored as 3 when they are in fact higher than that but the provider did not bother to actually assess it properly.
This may not always have huge implications for patient care, but it could potentially create the impression of improvement when there has been none.
-
 1
1
-
-
Thanks very much! Looks like I'll need to get myself a copy of that.
-
I did a search and came up with a few mentions of things relating to this, but not this exact question. I am looking for an ECG book that goes beyond the basics of interpretation (of which there are countless options). Which would you recommend and why?
Thanks for your help!
-
I'll add another thought on why calling OLMC is not idea (again, I'm not arguing with anyone following their own agency's requirements though). Say you call and describe a patient who has capacity but also a potentially serious illness or injury and the doctor tells you to bring them to hospital. What happens then if the patient continues to refuse? If the patient has capacity, this is completely wrong. Even if the doctor would take some of the blame in the end if the patient pushed the issue after having been somehow forced to go to the hospital, surely the EMS providers should also be to blame. I don't feel like "I was just following orders" is a good reason to violate a patient's right to autonomy.
-
Keep in mind that this is very location dependent, especially when you are talking about the US. In the system I grew up in, if you felt a pt needed to go and they wanted to RMA, you HAD to contact medical control and speak with the doc. It was a volley system so there really were no supervisors like you find in a paid system. I think in this case, you need to justify and document how the patient DOES NOT have capacity.
Yeah, I am not at all arguing what we might be forced to do but I just wanted to suggest that this isn't ideal.
-
-
If I were the on scene EMT running the call, I'd involve FIRST the OLMC Doctor, with all VS and observations reported. On request, I'd have the Doc talk to the potential patient. Dependent on the OLMC Doc's recommendation after speaking with the patient, I'd either get the Cop witnessed RMA signature, or the Cop's "Protective Custody" for the patient.
Either way, "document, Document, DOCUMENT!"
(Attention "Newbies": OLMC = On Line Medical Control)
Richard, while I accept that this may have been the practice for you, I disagree that this should be the standard way things work in an ideal environment. A competent patient can refuse care. If there isn't an issue of capacity then the patient can make an informed refusal and there is no need to call a doctor. I understand the desire to CYA, but I think that that is a poor reason to make us dependent on calling doctors. If anything, I would think it would be more appropriate to involve an EMS supervisor if you want someone else's name attached to things. But I do completely agree that no matter how it happens, this would need to be documented well, paying particular attention to how it was determined that the patient was competent and how the refusal was informed.
-
Well, for starters, there is no facility so to speak. We are going to kinda be out in the jungle. Well, not exactly jungle but most definitely coastal semi-tropics.
The gesture is not as admirable as you would think because I had not intended on giving it to them but simply keeping it on standby. I wish I had one to give away but then I would have to jump my patients with battery cables or some crazy thing like that

Is an AED even needed in the situation that you will be in? (That isn't meant to be rhetorical) I obviously have no idea what you're doing where, but I think that a lot of time the equipment brought overseas for medical volunteering doesn't line up with the local needs. Is there something else that might be more useful given the trouble that you may experience transporting the AED?
-
Am I willing to take responsibility for a full deaf partner who has to have me do any hearing based assessments, radio comms, and maintain full situational awareness for all of us? Man, that's a tough one. They better be one hell of a clinician despite the deficit.
I think this is what it really comes down to here. We sort of strayed from the original case where the EMT is described as "deaf" rather than having some type of deficit that is not complete deafness. This is all good for discussion, but if we shift back to talking about a completely deaf EMT, I don't see how we can justify having them work on an ambulance. I'd love it if we could accomodate everyone who would make an intelligent addition to our profession, but that just isn't how it works.
I like the question that you have raised though. How many people here would be willing to work with a fully deaf partner for your next shift? I wouldn't because I firmly believe that the patient would risk not receiving the care they deserve.
(aspiringemt, you keep doing what you're doing... I'm obviously not talking about a case like yours)
-
Congratulations! I can certainly appreciate the feeling of wanting more and sadly needing to move outside of our profession for that. I would be curious to hear more about your first PA job. I would be particularly curious what acuity of patients are you seeing and how much autonomy do you have, but any thoughts on your transition to the PA workforce would be interesting to hear.
-
If he's just providing a supine taxi service, then I guess there is no problem.
If he is doing real emergency work, then my thoughts on it would depend on what it means that he can "hear some" with hearing aids. As nice as it sounds for this guy to have a paying job as an EMT, if he can't perform the key functions required for it then he shouldn't be doing it. I am all for being inclusive and accommodating when possible, but a patient should never receive compromised care because of it.
-
At my college we had old clothes that we would use for trauma scenarios to actually be able to cut clothes to expose things (not all of the time, but usually during testing). It may seem like a little thing to worry about practicing, but I think the more realism we can have in scenarios, the better. Maybe there is a similar program near you that you could trust to use to cut them up in scenarios like this?
-
This is definitely something you will need to investigate and find a reliable answer to before beginning school (more reliable than we can give you on here). To work in Ontario, I had to prove through blood tests that I had received the MMR vaccine and it worked (I suspect that this is dictated my the Ministry of Health, but I don't have the time at the moment to try to look this up).
It turned out for me that my immunity was actually not that great to one of them so I had to go back and be vaccinated again. So my concern for you would not be about a specific allergic reaction but rather that you have immunity to these things. I don't know whether there is any flexibility in this or what your other options might be in terms of immunization.
You also mentioned paralysis. If there are lingering effects from this that will affect your ability to lift, then that will be an even bigger deal than everything else. Sometimes we don't think too much about that part of the job when entering a paramedic program, but it is one thing we do on nearly every call. If you can't lift, you can't be a paramedic.
As mobey says though, get in touch with your program coordinator (Mary Osinga, 705-749-5530 ext. 1733 or mosinga@flemingc.on.ca). Don't trust anything that any of us have told you here. Even when getting information from Mary, be absolutely sure she is giving you genuine answers that can be backed up with documentation and if not then seek answers elsewhere. Something that could prevent you from having a career after two hard years of school is important to figure out now. I'm glad that you're trying to do this!
Good luck! And congratulations on getting into a paramedic program.
-
1
-
-
Also, unless I missed it somewhere, it seems like we're making some really big assumptions of this patients weight based on a description of "obese"
ShareObesity is an abnormal accumulation of body fat, usually 20% or more over an individual's ideal body weight.
If her ideal weight is 100lbs, and she weighs 125, correctly identifying her as obsese, then I think that many of the assumptions that have been made based on her weight would be illogical, right?
-
I think that the more important thing that the stethoscope side of things is knowing the anatomy and putting the diaphragm/bell right over the artery rather than just sticking it somewhere in the antecubital fossa. I strongly suggest taking the time to palpate the brachial artery to get this exactly right (and I do do this myself), but if you're not going to do that then you should at least know where the brachial artery lies. It is more medial rather than in the centre where many people seem to stick their stethoscopes before complaining about how it was such a difficult BP to obtain.
-
Too bad it is Americans only! Good luck!
-
This is a doctor at a SNF. Who knows what protocol they use to determine death. A strip would want to be seen by the docs. I have yet to see a SNF have a 12 lead. Obvious signs of death excluded, this is a case that would require at least a strip sent to the Medical Control doc to make the call. Just because there is a "doctor" on scene doesn't automatically grant him the authority.
Why are we calling the doctor a "doctor"? Did I miss somewhere where his credentials were questioned? A doctor does have the authority to pronounce death and they are certainly not required to following any ambulance services protocol for how they do this for their patients.
-
Thanks guys. The way they phrased it in the email from them I wasn't sure if this was something that I was in a position where I need to negotiate to get something fair, but it sounds like what I have been offered is decent so I will go with it. Thanks again.
-
Hey guys,
I am just hoping to get some feedback to know whether what I have been offered is fair for an industrial day rate for an EMT-A in Albera. Is $350 a reasonable rate to work for a company with a good reputation?
Thanks!
-
As others have said, there is nothing to discuss. The patient is dead and there's nothing we need to do.
Cadaver, Anatomy, and Procedure Lab for EMS December 3 and 4, 2013
in Education and Training
Posted
That is great news! I'm glad we haven't worn out our welcome yet.
For anyone who isn't sure what this is about, hopefully a search will reveal the threads from every year since 2008 (wow!) when 'zilla has been nice enough to first invite us. It is a truly amazing learning opportunity that you are unlikely to find anywhere else. Not matter what capacity you work in, you will learn something. And the lunch is pretty good too.