


akroeze
-
Posts
1,205 -
Joined
-
Last visited
-
Days Won
1
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by akroeze
-
-
Don't carry it, never have.
-
Man who does this JBan guy think he is? You talk a lot of BS you must be a fireman.
If you don't have anything to contribute I suggest you find a new forum to post on. Posts like that contribute nothing to the discussion and only create problems
-
Further to that, if you are unable to remove the obstruction with direct visualization you should consider actually pushing the foreign bolus FURTHER down with the ETT in hopes of forcing it into a mainstem.
-
Same offer as Jake, I'll have my car there.
-
This image is the best one I could find. My ex partner there is showing what we commonly wore in the extreme northern Ontario service I used to work for. And that was nearing Christmas time so it was bloody cold. A sweater with a wind breaker is all you need for 95% of your calls.

-
XL
Unfortunately as I have yet to regain employment I won't be able to get service specific gear
Also, could everyone post their hotel that they are staying at? I want to try to stay with the group... makes things easier.
-
I have my theory that jban is trolling in their own way. The posts are just enough to incite a response out of people.
-
It's my understanding that York Region EMS uses them and I'm pretty sure Toronto EMS is as well since their CME for their FD First Responders includes posters reminding them to put it on. I assume that's all under ROC though; since just about everything else is in Ontario.
Windsor-Essex is using the ITD (or a sham) as part of the ROC study.
-
So crotchity, what I got from your post is that you need to be able to show up other providers in order to enjoy your work?
-
I'll play devil's advocate....
Why does all that matter to the individual doing the work that he is the only medic in the region? Doesn't that mean that he has a better chance of getting a high volume of high acuity calls (which is what many want)?
-
Did you by chance mean to post that in the blog there on your profile and accidently made a new thread instead?
-
Just curious... you're aware of the low, low, low, low pay that they have there right?
What level are you and what province?
-
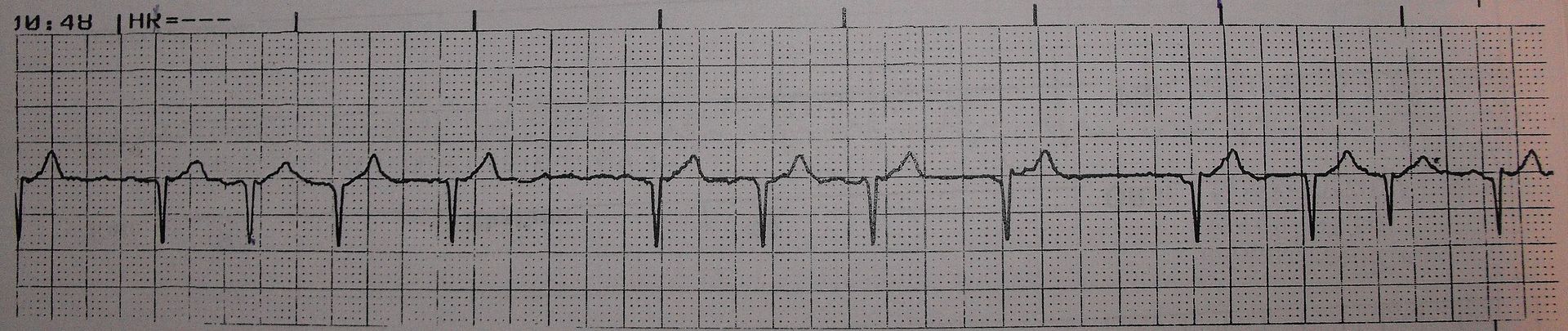
I think the idea of flutter with fib as well is probably the best option with the given strip.
I think the moral of the story is that this isn't the best example of a-fib to put in an "introduction to rhythm interpretation" booklet.

-
As discussed, as restitution you owe me a Pepsi if we ever meet
-
But the definition of a-fib is irreg irreg with absent p waves isn't it? This is absent p waves with reg irreg
-
Happy birthday!
me too
-
This is all I have. It is part of a package that my gf (in Primary Care Paramedic school) got for ECG interpretation teaching. They are calling it A-Fib.... I disagree. There is no 12-lead, no other leads, no history. What you see is what is given.
I don't call it A-Fib.
Every block of 4 beats the first 3 have identical R-R to each other then the fourth is delayed, perhaps an escape beat.
I don't know what to call it but it isn't A-Fib
-
http://i147.photobucket.com/albums/r298/akroeze/ECG.jpg
Not sure if I'm looking too much into it or not but there seems to be more to this than first meets the eye. Measure out the R-R intervals for the groups.
-
you bady mass index stuff.
I'm sorry... did you just call me bad?
-
I am by no means an expert but the rotor wing aircraft here in Ontario do no scene calls at night. As in none. The risks are too great.
They will only land at designated spots (eg helipads).
-
Since we're on the topic, anyone know what might be found in "Difficult Intubation Kit"? They called for it in the ER the other day...someone had to go to some special supply room to get. Only some of the ER staff even knew they had one, so not even used for most difficult intubations... I know LMA was in it which I think he used in some creative manner to get the ET tube in...
Google Intubating LMA.... they're pretty cool.
-
If I could change something about EMS, it would be to require nursing students (particularly RN students) to do several ambulance ride-outs as part of their clinicals. We often have to do several ER and hospital clinicals and that gives us an understanding of what their job entails, but they often don't know anything about what we do. Unless they are EMS trained too.
It would never solve the problems everyone runs into in the ER, but maybe if they had to go through some of the things we go through out there, they would at least understand why we are grouchy/wet/covered in blood/or just having a bad day. Maybe if they were on a multi-car pileup and had to do all the work themselves prior to other units getting there, without techs/docs/housekeeping/other nurses to help out, they would be just a little more with it on why we never quite got that laceration all cleaned up. Maybe at the least it would be better than nothing at all.
How many nursing home shifts did you do so you understood why it is that you are greeted the way you are when you go to one?
-
In addition to the above critical points made by others (see, I captured the OP and valid responses) I do it because in the past, people have denied saying certain things. When I went back to show them they did indeed say something, I have found either the entire post gone OR they have edited it and changed whatever we were discussing. We have since implemented some safeguards against that practice, however it is still nice to copy for any of the above reasons.
The only time I detest someone doing it, is when they have nothing of value to add. They either thrown in 1-3 words or a simple smiley face at the end of this long discussion.
8)
-
Isn't that a good 1/2" more than you need?
I don't have the studies in front of me but there was a study done that showed that the needles we use are often not long enough
{kind=link}
southwest ambulance, arizona?????
in General EMS Discussion
Posted
WHY ARE WE YELLING?