


wrmedic82
-
Posts
171 -
Joined
-
Last visited
-
Days Won
2
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by wrmedic82
-
-
Never heard of that... learn something new everyday.
-
May I recommend instead of becoming a EMT, try being a EMD . As is we drive dangerously in our everyday job, its inevitable. Everyone here that drives an ambulance does whatever it takes to ensure that as we are running code, it is done as safely as humanly possible. But when those lights and sirens are kicked on liability, and a chance you could be in a wreck increase greatly. People don't pat attention, and then you hit them or they hit you. Some states say that running lights and sirens does NOT give you the right to push people out of the way or have people stop for you to go through an intersection. They are viewed as courtesy lights and say to proceed with due regard. Meaning, if you blow through an intersection lights and sirens, the lights red, you proceed through and somebody hits you. Your At Fault. They may get a ticket for failing to yield right of way to an emergency vehicle, but you get cited as well.
It takes alot of sound judgement to do this job whether you are doing patient care or getting the patient to the hospital. And everybody at one time or another has had a lapse in judgment. But with this job its critical this is minimal and that everybody goes home safely. As said earlier you may find it hard for the next 5-7 years to get on with a ambulance service because they run background and driving record checks.
Another thing I would do before paying for your EMT class is to call the state health service that governs EMS to see if they would even certify you after having that charge on your record. It would suck if you invested the time and money into EMT school just to find out the state will not allow you to practice EMS due to the charge on your record.
-
Bad Advice Man takes a transfer
Disclaimer - For those who know, and those who don't, Bad Advice Man and DG are completely imaginary characters. These stories have no basis in reality and are completely made up. There is no chance ever that you or anyone you ever have or will know has or had anything even remotely similar occur. Even if you THINK you know who and what they refer to, you don't... Attempted duplication of any event in any BAM story is likely to get you fired, thrown in jail, or shot.... or some combination thereof... you get the point.
That being said....
...........................
It was a beautiful spring day. The sky was blue, the temperature was perfect, and the flowers were blooming. It was a perfect day to be at the lake.
Unfortunately, dispatch thought it was a better day for a transfer.
"Medic 34, copy call"
Bad Advice Man, EMT-P and Delusions Galore, EMT ignore the squaking contraption mounted in the console and continue their safety check of the local park.... Apparantly college had gotten out early that day... and tan had become the new black.
"Medic 34, copy call"
EMT Galore grudgingly grabbed the mic... "Hi, you have reached Medic 34... we aren't in right now, but if you will leave your name, number, and a short message, we will get back with you later.... "
"Medic 34, you have a call" the black box squaked back.
DG didn't miss a beat. "The unit you have called... Medic 3...4 has been changed... The new number is unlisted at the crews request..."
Bad Advice Man sets down his 50x binoculars to check his pager. "Very funny.... " which was immediately followed by the call information.
Luckily, this one would be an appropriate use of BAM's years of experience, a real call requiring thought, medicine, differential diagnosis, and skill. "P-5, Physician's hospital going back to Southern Care Center.... DX - r/o fever"
Medic 34 arrived on scene with exactly 3.2 seconds to spare before it became a delayed response and checked on scene. Rolling in with an empty cot made the ER staff extatic, and, of course, allowed just a little extra time to socialize before the long ride to the 4th floor.
As our heros passed the nurses station on 4 east, they heard what could only be discribed as snickering. The cot stopped.
"What's so funny?" BAM asked.
Nurse Kelly smiled. "Oh... nothing..... your patient is in 423" She handed the dictionary of useless paper to BAM and signed the "Astonishing Contraption of Silliness" on behalf of the patient.
The room was standard decor de hospital, white with hints of poo-green and vomit yellow, the simulated wood-grain formica furniture laden with bins and paste and other accessories. Through the window, BAM gazed longingly at the park he had just left and then turned to the patient who was laying, head elevated with her fists clenched.
"Well hello!" BAM said with a cheery voice.
The patient replied the only way she could. "You're standing there..... You're standing there.... You're standing there..... You're standing there.... You're standing there..... You're standing there...."
The repetition continued over and over....
... and over again....
"Yes I am" BAM responded.
Ms. Jones (the patient) clenched her fists tighter, pumping them with each short sentence.... "Yes I am.... Yes I am... Yes I am...."
EMT Galore stated the obvious. "Wow, that's like Steven Hawking arguing with a talking clock..."
As BAM turned toward his partner, in walked the lovely and talented Nurse Betty, obviously to give report. (This WAS after all, a transfer of patient care).
"Yes I am.... Yes I am... Yes I am...."
"Well hello Nurse Betty" BAM said with a smile.
"Yes I am.... Yes I am... Yes I am...."
Nurse Betty looked into BAM's eyes and in a way that was somewhat... different... than normal... "Hi BAM .... Hi DG..." She never took her eyes off Bad Advice Man.
"Yes I am.... Yes I am... Yes I am...."
As she moved forward, Bad Advice Man felt that spring might be getting the best of him. The repetative sounds of the patient were gone... His attention completely taken by the angel in blue scrubs. Nurse Betty moved slower, almost slinking as she approached the bed. Their eyes never broke contact as she came closer. It was hard to ignore her presence in any room, but this time it was the details... the way she moved, the way she was smiling, the look in her eyes..... BAM made a mental reminder to stay professional...
The smallness of the room only placed emphasis on how close she came to him, their bodies nearly touching... her piercing green eyes burning into him... She turned her head just slightly sideways and leaned into him... her lips opened and she whispered two words...
"Watch this...."
Nurse Betty turned to Ms. Jones. "Rock-N-Roll"
It was at that instant that BAM was completely cured of his spring fever... and, for the time being, his thoughts of Nurse Betty... It was as if the room had been transformed into a KISS concert, where Ms. Jones was the only spectator.
"Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll!...." The patient continued, yelling the phrase without end... "Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll!...."
"Have fun!" Nurse Betty said as she left the room... BAM realized that the look in Betty's eyes had been one of deviance... And, for some reason, he found himself not surprised....
Holding in their laughter, BAM and DG lifted the patient to their cot, timing the movement to the pumping of 84 year old fists... "Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll!...."
DG lead the way as they rolled down the hallway toward the elevator....
"Rock-N-Roll! Rock-N-Roll! Rock-N-Roll! Rock-N-Roll!...." Ms. Jones never gave up on the last encore....
BAM waved politely at the nurses on the way by.. "Thank's guys.... Thanks a lot..."
EMT galore turned quickly toward the desk as a doctor actually fell out of his chair in a fit of laughter.
During the ride down, Paramedic BAM considered the options for the return to the nursing home.
DG, on the other hand was less helpful. "Gimme a beer" He said to Ms. Jones.
"Gimme a beer! Gimme a beer! Gimmie a beer!...."
Bad Advice Man became acutely aware of the patient's conditon... Unfortunately, so did DG.
The walk through the ED was considerably less social. "Gimme a beer! Gimme a beer! Gimmie a beer!....
Gimme a beer! Gimme a beer! Gimmie a beer!...."
Again, another laughter related injury. BAM realized that remaining in a public area would result in an unexplainable MCI.
Loaded in the MICU, DG decided to drive the short trip to SCC.... but that didn't keep him from interacting with the patient. "Ozzy rules!" he yelled to the back.
"Ozzy Rules! Ozzy Rules! Ozzy Rules..."
BAM knew he had approximately 5 minutes to come up with a solution... that wouldn't involve a complaint... and DG wasn't helping.
"Dude, give me a break here!" BAM shouted to his partner.
"Give me a break here! Give me a break here! Give me a break here! Give me a break here! ..."
DG didn't agree on the care plan... "SLAYER!" he yelled back.
"Slay-er! Slay-er! Slay-er!...."
Bad Advice Man tried to control the situation... "Shut the F up DG!"
"Shut the F up DG! Shut the F up DG! Shut the F up DG! Shut the F up DG! ...."
BAM realized the severity of the situation and explained it to DG... (as if he didn't know already) "Dude, cut it out... we are gonna get fired...."
Delusions Galore agreed, if only because he understood that "Park Safety Checks" were slightly less cool when you are unemployed...
Bad Advice Man weighed all his options... He couldn't change the patient's condition or take her back to the hospital... Finally, he thought "What can I get her to say that won't get me fired?...."
He looked Ms. Jones in the eyes and said with authority: "I'm hungry"
"I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry..." A weight lifted from our heros as they checked out at the nursing home....
Rolling inside and up the elevator, Ms. Jones continued saying her mantra: "I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry!"
Entering the room, they moved quickly, transfering her to her bed... BAM and DG both hinted about the hospital... "Must not have given her lunch... Been this way since we got there... I'm kinda hungry myself...."
It worked....
BAM and DG moved quickly (without being too obvious) to the elevator... The discussed what they were going to have for lunch, and later for dinner....
In the background, Ms. Jones never stopped... "I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry! I'm hungry!"
With the code entered in the keypad, BAM and DG waited nervously for their escape capsule...
From the end of the hall: "I'm hungry! I'm hungry! I'm hungry....."
"Ping!" The elevator chimed as the elevator arrived on their floor.
As the door opened, in the distance, they heard what was, quite possibly, the loudest yell ever heard in a nursing home....
"ROCK AND ROLL!"
Pushing the cot inside, the elevator door closed to the sound of running footsteps... the kind made by 120kg of pressure in oversided "nurse shoes"... followed by banging on the exterior door of the elevator as they decended....
... BAM and DG made their egress to the MICU with record efficiency... as if they were Secret Service Agents protecting the Presidential Cot.... Getting ready for the next call would have to wait.... until they were around the block... behind a building.... and under a tree....
... DG stated the obvoious... "That was close.... " as he turned on the FM radio...
And with serendipity that can only be explained by a room full of nerds versed in chaos theory, a song started on the radio....
".... I.... Wanna Rock-n-Roll all night..... "
-
I'd let an older woman touch me too if there was a meal involved....
Especially if the older woman can cook.. Im a sucker for some good ole home cookin.
-
My feeling on lights and sirens is this. Or me putting my foot in my mouth.
As far as response
Follow department policy as far as the use of lights and sirens. Its just good CYA.
As far as transport
Use common sense and sound judgment. Err on the side of the patient. Alot of times lights and sirens will add stress to everyone involved. As a rule of thumb on our truck if there is no compromise to ABC's and indication of CVA (provided the patient is a possible candidate for fibrinolytic therapy) we will not run hot to the hospital.
As far as driving
Driving to and from the scene should be done with as much sense of urgency that keeps both yourself, and everyone safe.
Be careful, be safe.
-
Some pictures I ran across.


-
That was great

-
www.half.com
-
Like everyone else says get checked out. The injury could be a simple muscle sprain to a disk problem in your back. Hell you may even learn something about yourself that you didn't even know. When I hurt my back last year, I discovered that I had spina bifida oculta. Although supposedly benign, the doc told me Id have to watch it from here on in.
One practice to get into is lifting with your legs. I had to for a while use a back brace to remind me to lift with my legs. Its doesn't completely prevent improper lifting. Just an idea. Its a bad habit to get into so break it sooner than later.
Good Luck
-
Me and my wife just has our baby boy at 12:31 this morning. He weighed 5 lbs 4.1 oz, and was 18 in long. He was 34 weeks and 1 day along. Couple funny things I want to mention though.
1. 4/30/09 was me and my wife's first anniversary.
2. After enjoying a wonderful dinner at Romano's Macaroni Grill. My wife asked what we wanted to do next because she didn't want to go home to do nothing. So I mentioned putt putt golf. Only thing she asked was I placed her ball for her as she has hard time bending down because of baby. I said no problem. A little while later I noticed she was having contractions nothing regular. I jokingly said to my wife, "watch you break water while playing putt putt". My wife was like I could only hope as she was done with being pregnant. Anyways, we get to putt putt, and after 9 good holes sure enough, the water breaks.
The baby was breach feet down. They did a c-section, and now my love and bundle of joy is here. I will try to post some pictures up as I can get them uploaded.
Baby's Name is Kayden Maveryck Roberts ( middle name mom's idea )
Something did come to me while in the delivery room. Now keep an open mind, and note there is no factual basis behind this statement but makes sense.
There is a reason why dad's are more lenient than mom's. Mom has X amount of hours in labor, and payback comes back to the child lol.
Everyone Take Care
-
Just to add something to the mix.
http://www.essortment.com/lifestyle/homehealthwhen_sksk.htm
http://74.125.95.132/search?q=cache:GCh0Ze...lient=firefox-a
And yes I was joking
-
Well, if my home is involved in a fire, I have the luxury of a paid, professional FD to respond. They are well trained, as that is their JOB. All they do is train and wait for a fire, MVC etc. I do not want to wait with hopes that a crew will respond because it's 3 in the morning and they have to go to work in the morning. Even if/when they eventually respond, I want them to be trained as if they where professional FF's. It doesn't matter that you volly, the job is the same. If they don't want to be trained to the same standards as everyone else, maybe it's a good thing that they will have to fold and be replaced by a professional dept. I'm surprised the IAFF hasn't jumped on this golden opportunity to increase membership and the dues that come with them.
Here's the thing. Most (not all, relax) Vollie FD's are comprised of the "Good Ol' Boy's" club. Some only want to be part of the dept. for the social aspect of it. Other's are way to eager and have been known to actually start fires because they have missed the action. I think, as with vollie EMS dept.'s, the end is near.
I fully agree with you jake. In a perfect world all fire personnel (volly or pro) would be trained according to NFPA 1001 FF1 & FF2. But with volunteers thats hard to do. Some departments are good about only allowing certified personnel on the fireground. others not so much. Sad but true reality.
-
http://www.sffma.org/smarty/index.php?page...tion#objectives
I can see both sides of the argument here. on one side most volunteer departments struggle as is to get the minimum training complete for firefighter basic with current planned training that maybe once a week (4-5 hrs a session). Adding additional required training hours may further hinder the amount of manpower on scene which is already stretched thin. On the other hand I could also see how increasing training in other areas could prove beneficial. It will be interesting to see how this plays out.
-
Just what I would do.
1. Advise dispatch that I was involved in MVC, and will need another unit to continue transport.
2. Assess the scene and advise if additional resources are needed.
3. I would not make any statements that could be construed as admission of guilt, thats PD's Job
4. Treat patients according to mechnism (which is low in this case) and chief complain.
5. Provide pertinent information to incoming units.
6. Transfer the most critical patient ( in this scenario the one inside the ambulance).
7. If no one wants to be transported, have the patients sign AMA or release at scene.
If they want to be evaluated, prepare patient for transport once additional unit arrives.
8. Stay onscene while PD does their investigation.
9. Do whatever company policy states. (i.e. Written statement, wee wee test ect)
10. Enjoy the rest of the night cuz its down hill from there.
-
Why do you want a child?
Robert, Why not? (kicks robert in the shin)
Congrats to you and yours. I know a great place to buy a shotgun when you need it. Take care
-
The "Hand Drop Over Face" technique I've heard of, not so the alcohol up the nose. Besides, as I'm BLS, per protocols, I don't have access to a syringe.
New York State DoH outlawed "Ammonia Inhalants", sometimes called "Snappers", over 30 years ago. Does anyone have them still included in local protocols? Please give the area/country, if you do, just for my own interest and curiosity.
We carry them on our trucks, and work great with hispanicus Panicus.
Ft Worth, Tx
-
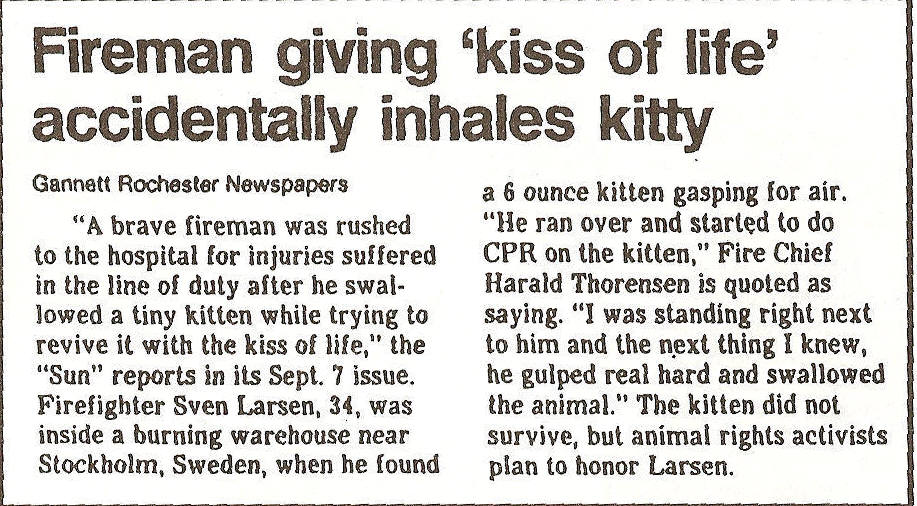
makes me want to run a couple miles, shed a couple pounds, and be pessimistic of save the world groups.



-
I think the old worn saying says it best. Treat the patient, not the monitor. Common sense is also key.
-
I for one would like to know what this mystical 'exception' to the law is. Since the patient was being seen for psychiatric problems, I would be curious to know how it affected the patients competence in this matter. I'm also curious as to how your local protocols define abandonment, and what they say about refusal of care.
Did the parents have guardianship or conservatorship over the patient? Had the patient been found mentally incompetent in a court of law?
The etiology/pathology of the seizures is irrelevant. The main point is that since care was terminated without the proper transfer of care to someone with an equal or higher licensure, the patient was abandoned. Let's not 'muddy the waters' by throwing etiology/pathology of the seizures, or a discussion of the patients medical history.
Couple things:
To answer your first question I don't know hence why this topic was brought up here. The whole point of this discussion is so I can see if there was something I missed. I have never heard of anything like this.
Second, if your read the beginning of the discussion I have already specified that no durable POA was presented by the parents on scene.
Third you are correct, etiology/ pathology is irrelevant. But again if you read the other posts you would see I was merely filling in the blanks as far as questions being asked in the discussion.
I will say this though. The real issue is not that the patient was turned over to family. But rather how it was done. That is where my problem lies. I know this is going to stir up a hornets nest so let me explain my side, and I will try to play medic advocate.
First and foremost I wouldn't have had the parents sign without a durable medical POA. That's something Ive known since I was in basic school. that was covered also in paramedic school which Im still currently in.
Second I would have personally conferred with the patient's neurologist. Getting his knowledge of the patient's Hx. Then provide the doctor with information gathered on scene, concerns, and any other pertinent information. If the doctor states that transport is still unnecessary at that point, then I would document the conversation in the chart including the physicians name, and DEA number. That way if it did come up in a legal setting it is documented, thus shifting liability to the neurologist.
Third if the later was not done. I would have at least waited for the patient to return to their baseline. Then advise the patient of risks and benefits of being txp. Then its up to the patient, and they can sign for themselves. Now Im not advocating doing this as it can take some time on scene for this to happen obviously. However legally would have been right. Reason it is because the patient that knows their own medical hx, what has happened, and is AOx4 which makes them legally competent. The law the places this under expressed consent. That way issues with all others involved are settled w/o conflict.
I am sure that the medic was thinking " well the parents and the doc don't want him to be transported so it would be ok to leave the patient with the parents".I'm also sure he meant well when doing what he did. Mom also stated she is a RN so the patient wouldn't be in unknowledgeable hands. Now am I saying this line of thinking is right?Can be if handled correctly as specified earlier.
Last I feel like I am beating a dead horse when I say I have contacted the medic involved, a supervisor, and our medical control (EPAB). All parties have been contacted, and know of the situation. Yes there was a delay in contacting EPAB. That I have no control over. It would be crazy to pull a emergency physician taking care of patients to get on the radio to handle a medico legal dispute.. All the physician is going to do is say contact your medical director. ( yes this has been done before, just different issue )
Lets keep this discussion civil.
-
Thanks for all your comments. They were about what I expected. I will need to fill in further on some details of the call.
Prior to leaving the scene:
I did contact a Supervisor /FTO(whom was in the truck) When I was told that the parents can sign on behalf of the patient. From the way it was told to me according to him that there was some type of exception to the rule that I was never aware of. The willingness of the supervisor to condone this action lead me to believe that this was acceptable. (not saying I agreed with it). The only form of online direction we have is base station physicians at the emergency rooms. Due to policies we have to direct disagreements to the supervisor. Most communication in our system to med control is via email, and voice mail.
The next day I approached the medical records manager concerning this matter to see if I could get a deeper explanation. He told me about what everyone here has said. Needless to say medical control ( EPAB in our system) was promptly advised of the incident and is currently under audit.
There really isn't a good reason as to why we didn't get a BGL. For that I will admit fault, and agree it should have been done.
Thanks again everyone for your comments they are much appreciated
Ok...I had to re-read the initial post before I felt ok to comment. That being said, most of what I have to say has already been said about POA/HC, etc, parents can't legally sign for him blah blah blah. So here's my question...why is his liver chirrotic? I would assume ETOH abuse? If that's the case, is the HX of SZ from DT's from past attempts at quitting? If that's the case, and the bleed is from a head bonk, and this SZ is from DT's, then it was a definate medical emergency that was abandoned. If not...still should have been transported, parent's wishes be damned-cause they can't sign (he's a big boy, no matter what mommy wants to think). Just my thoughts and/or questions.Patient also had Hx of Hepatitis C. Patient was being seen for psychiatric problems from what Ive been told. No known alcohol abuse specified onscene by therapist, and family onscene. And I agree that he should have been transported, or at least given enough time to return to his baseline mental status and base txp based on the request of the patient.
-
If you double click on the strip it gets bigger.
-
I don't know about the actual laws in your state, so I will answer this question the best I can based on my experience and how I would likely do things if I were on the call.
In my opinion, nobody can sign a refusal FOR an adult patient unless that person has a legal power of attorney. It doesn't matter if they were his parents, your patient was an adult who makes his own decisions regarding his health care, and he was not alert and oriented enough to understand the consequences of refusing. I also feel like the doctor on the phone is irrelevant. You don't work for him or under his license, and he wasn't present to assess or take care of the patient. In my opinion, it really doesn't matter at all what some other guy on the phone believes about your patient. He's not there.
If the parents were going to make a big fuss if you attempted to transport, I would have got my medical control on the line and let them hash it out. Leaving this patient behind with a refusal signed by someone other than the patient him/herself or a POA is not a decision that I would want to bear on my own. I would involve as many other people as possible: medcon, supervisor, police, etc.
By the way,
lol, what?

The patient's iris and pupils were going side to side in a rapid manner. Kinda cartoon like. But this was a new finding because his eyes were not doing this inside the office building.
-
Thanks for standing up for those who cannot stand for themselves sometimes.
I a very familiar with this topic as well...There are those of us (survivors of such addictions as cutting, true cutting not just for attention) who get "caught" just as we are slipping away. If you can talk to them and let them know that they are free to talk it really helps. And you should also know that if caught AND properly treated they can live a normal healthy life. They are human beings with feelings just like anyone else, so please don't judge them, it will only make it worse.
Agreed
-
We responded to a call at a therapist office for a 35/m who had a seizure. Upon our arrival at the patient's side. The patient was found sitting in a chair receiving supplemental oxygen via NC 2 L/min from our firefighter first responders. The patients parents were onscene when we arrived, and did not want their son transported to the emergency room. I personally advised the mother about the needs, risks, and benefits of going to the hospital. Mom didnt budge. Meanwhile the patient is still comming around but still obviously post ictle( not answering all questions appropriatelu). Vital signs were HR 90, RR 20, BP 130/80, SpO2 97% eyes were initially 3mm PEARL, unknown AO status as my partner who was running the show didnt care to find out .PHx seizures, brain bleed secondary to a seizure, cirrhosis of the liver. We did not obtain blood glucose. Parents state that they will call the patient's neurologist to get his opinion. Mom goes into the therapists office and makes a phone call. Shortly after mom returns, and says the neurologist said no that the patient did not need to be transported. No verification was done on my partners end ( as he was running the call) Parents did not have a medical power of attorney with them. My partner had the parents signs AMA, and released the patient to the care of the parents. While we were assisting the patient into the parents car, I noticed that the patients pupils were pinging, and patient began to exhibit lethargy.
Now a couple things didn't set right with me, and I want to see if maybe Im being too hypercritical or if Im right to not feel right about this.
1.If the patient is an adult, normally AOx4 confirmed by parents, and is confused due to seizure. Can patient be legally turned over to parents in the absence of medical POA??
2. If parents talk to patient's physician concerning txp, is it prudent for the medic onscene to make contact with the physician?
3. With the lack of medical POA, unconfirmed request by patient's physician, and the patient obviously confused. Would you have made transport decision for the patient on the side of the family's request or the side of the patient.
The responses I got from the medic I was working with was that the decision was on the side of the patient, and that the parents can sign on behalf of the patient, and hold up legally. (not sure I agree with that, but I dont know)
What would ya'll do?
What insight do ya'll have to offer?

Transfers vs. 911
in General EMS Discussion
Posted
Ok I haven't put my foot in my mouth in a while so here it goes.
I'm kinda riding the fence on this topic. To a degree if a patient needs ongoing medical treatment during transport to point B. Then the ambulance is the way to go.
On the flip side.
Do I feel dialysis patients needing just a ride need a ambulance.. that can go 50/50 depending on PHx, and medical needs ( i.e. oxygen)
Do I feel that a patient that is cleared by a medical doctor to go home needs a ambulance..No
Do I feel psych transfers that require no, or expected by a physician to not require treatment en route need a ambulance..No
There are good arguments for both sides don't get me wrong. But where I draw the line is when no medical necessity is required, and using trained professionals as a taxi service paid for by tax payers. Luckily in our area we have a company that handles non-emergency transfers for patients that require no medical necessity. These people may only have CPR training. The state does set requirements for this service and what they can and cannot transport. Ultimately this helps to reduce the load on our already busy system.
That is my 2 cents