


wrmedic82
-
Posts
171 -
Joined
-
Last visited
-
Days Won
2
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by wrmedic82
-
-
This is just my own personal rant.
In Dallas, EMS really has a bad rap. This of course does not come w/o merit though. We have alot of EMS providers (EMT's and Paramedic's alike)just not caring or not seeking knowledge to better themselves and their patient care. As a result comes very basic protocols to reduce liability, and lowered standards of patient care. It is a shame. When I got into this, I wanted to give 100% when it comes to patient care. I never wanted to be the EMT that only knew what was taught in school. Now as the end of paramedic school comes closer to an end for me, I am learning from the doctors I work with at the monitoring center where I currently work.
I do not believe EMS can move forward in a direction in which we want unless we take what we do seriously. (please do not interpret "seriously" as you have to work with a pole up your butt) Only when pro's in the medical profession see that we know what we are doing and then some can we move truely past "ambulance drivers" or "knowing enough to be dangerous".
-
 2
2
-
-
LMAO priceless
-
This is discriminatory thinking just as much as the double female staffing...what exactly constitutes a male or female issue? Are these call outs so common that there is a need to have a male or female depending on the sex of the patient?
Are you saying that as a male I can not effectively treat a female "problem"? Are you trying to say I could not deal with an OB issue/delivery/complication, a sexual assault, bacterial vaginosis, STDs, unusual discharges, lump in the breast? What are you going to do that is any different than me simply because you have a vagina and I don't?
I can talk about and handle any of these issues with professionalism and empathy. Prehospitally or more specifically on an ambulance, the treatments will not change based on the health care provider's sex. On the flip side are you saying as a female that you could not handle ED or penile discharges or male sexual assault?
Because short of sexual organ dysfunctions or OB, there is no difference between male and female EMS issues and there is absolute zero need to have a male for male issues and female for female issues. That is one HUGE step backwards for medicine overall and an extremely narrow minded point of view.
I think she has a valid point. Take for instance the muslim culture. Did you know if a male healthcare provider touches his wife she could be killed? Granted this is the US and those actions may not be premissive per se, but for those who are dogmatic (radical islam) that may not matter much. Also if a woman goes to treat a male who's culture is that the man is in charge may hesitate, or refuse transport or treatment. It would be very callus for us to say " well fine don't go with us" and go on about our business. This also of course can or will violate the first rule of medicine do no harm. For that I do not believe her to be sexist but rather a realist.
As far as lifting goes, I hold women I work with to the same standard as myself. Yes I can lift alot of heavy patients and have throughout my career. I have also lifted people I should not have w/o assistance. So with pride and ego aside I hold them to that standard. If they cant lift they do not belong on a ambulance period. This goes for males and females alike.
-
They had no right to the info, whether it starts a battle or not. DPS administration would not take a kind view on the actions of this trooper when they found out the legal ramifications.
Just throwing this out there. How did the trooper know that the ambulance was transporting a patient vs. an illegal alien vs. a fugitive? How could he/she verify that the ambulance crew was not transporting someone that was wanted? The ambulance out-of-state deal could have been a cause for suspicion. And who knows if rescue randy did not call something in or if there was a code silver and the trooper was making sure that the elderly patient (if they were elderly) was not the one they were looking for?
I personally would comply because you really have no idea what they are looking for, nor is alot of officers going to tell you which has been my experience.
-
Short and sweet: In a situation of a trauma patient with increased intracranial pressure(ICP), would a supraglotic airway (i.e. king, combitube, LMA, etc.) cause a greater increase in ICP (say, compared to laryngoscopy and ET tube placement) due to its constant pressure on pharyngeal structures?
Back story (for those who are interested): In medic class we were discussing a scenario of head trauma patient (I'll leave out the details for now and add them later if they become pertinent) who seemed to be decompensating and required airway management. The area I'm in is largely advocating the use of supraglotic airways over intubation in the prehospital setting and I asked if a supraglotic airway would be problematic in this situation as the sustained pressure would might a more significant increase in ICP over the breif pressure required to use a laryngoscope and intubate. My instructors were unable to provide an answer so I figured I'd pose the question to The City.
Thanks in advance for any enlightenment anyone can provide.
This is my take. If you have to take over someones airway in the trauma setting, the question you should ask is which airway is the most appropriate? Most people would agree the the ET tube is the way to go because its more secure. And I completely agree. However the longer it takes to intubate your patient the higher the likelihood of increased ICP. So my view on supraglottic vs. endotracheal is which is quicker to obtain in regards to which airway is appropriate. With easy airways I would happily go for the ET tube, however for more difficult airways I prefer not fumble around trying to get the tube due to risks involved and go for a king (my personal preference) or combitube.
-
Here is the link to a site by Dr. Frank Yanowitz. Dr. Yanowitz works with our company to assist us on abnormal ECG. He is a expert in the field of cardiac electrophysiology.
-
I will agree with 3rd degree AV Block w/ Left Bundle Branch Block.
Here is my evidence
The atrial rate is about 50 bpm
The ventricular rate is 30-40 due to some irregularities
There does not appear to be any relationship between the P wave and the proceding QRS.
If you look at the 2nd beat the QRS is a little different than that of the rest of the other beats in lead II. Chances are the P wave is buried within the QRS. Also the 3rd beat look at the T wave. It is different from any of the other T waves. More than likely again the P wave is buried within the T wave.
The widened QRS with downward deflection in V1 makes the diagnosis of Left bundle branch block. Recall a normal QRS is <0.10 sec or 2.5 small boxes.
With this evidence its safe to diagnosis this as 3rd degree AVB with LBBB
Hope this helps.
-
I'm not exactly sure what you mean by "teching" the patient. As kinda a just that I have gathered you had a patient that could not fend for themselves and you did not feel right leaving them at home when you know they are going to be alone for the most part with the exception of when the aid is present in the home. Please correct me if I'm getting the wrong impression.
If my impression is correct then I have a couple thoughts.1. There is an old addage you can lead a horse to water, but you cannot make him drink. I won't argue that the patient probably should not be left alone at home in his state. However if he refuses provided he can legally make decisions, then you have to respect their wishes. Situations similar to this happen all the time. The ethics debate usually ends with patients rights. To go above the patient, you would need to get something from the court. Otherwise it sucks but your at a loss.
2nd and I know this might sound like kicking a dead horse but provided they can legally make decisions they have a right to dictate their own care. Again sucks to be us sometimes.
And third and most important talk to your patient regarding your concerns if you feel comfortable and appropriate. Sometimes a second person stating the same thing as the physician and providing other angles to look at may prove to be beneficial. Just don't get into a arguing match. That will only serve to piss off your patient and get you nowhere.
-
1
-
-
Welcome from the DFW
-
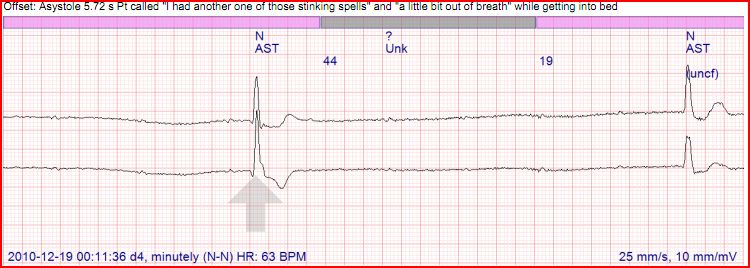
The answer to all of the above is Third Degree AV Block with IVCD. In the first strip as some have states there are P waves w/o a corresponding QRS. In short the P waves are doing their dizzle and the QRS's are doing their dizzle. But they aint working together fo shizzle. The first three strips was the actual onset of the block. As stated earlier, the original rhythm was First degree with IVCD. The IVCD explains the wide QRS. Thats why they are not PVC's but normal beats. Compare the beats on the 18 second strip to that of the picture on facebook. They are identical! Stay tuned I have another interesting patient coming soon.
-
Here is a link to my facebook page where the 4th strip is.
-
10 cardiologists would come up with 10 diagnosis', but I would call it third degree with conduction delay, regardless of what you call it, it is too slow and needs to be corrected immediately, so argueing over what it is really moot. What was the patients b/p supine and sitting ?
Unfortunately I cannot give you info on blood pressure or whether or not she had a positive tilt. This is due to me being in a monitoring center and not in the field at the moment. Dr was contacted immediately after the incident. The rhythm did speed up to 32-34 bpm. I would post that strip up but it would exceed the bandwidth.
-
The thread was for rhythm analysis purposes, however if you want to specify your course of treatment thats fine too. The main purpose is purely educational
-
I am not against homosexuals in the military. But I do have concerns on the basis of distraction, and losses of moral due to the distraction. As a general rule I feel what happens in the bedroom should stay in the bedroom and not be brought to the work place whether you be straight or homosexual. On the front lines sexual preferences should not be a issue PERIOD!
Some people do not accept people who are homosexual. I am not saying its right. But we all know the type exists.That is a reality we have to acknowledge. If someone who is a homophobe knows they are depending on someone whom they feel is attracted to them is in a life or death situation, they may not depend on that particular individual or isolate that individual that is homosexual. Again I'm not saying that it is right. But at the end of the day the question has to be asked did it effect the moral of the unit?.
Some people can "get over it" and get passed the individuals sexual preference which is mature, where as some may not and tend to isolate themselves from individuals that do not make them feel comfortable. That of course is problematic when you need a cohesive team for survival.
Those are my thoughts I wish all well.
-
I will add that after this episode, the patients HR stayed between 32-34 bpm.
-
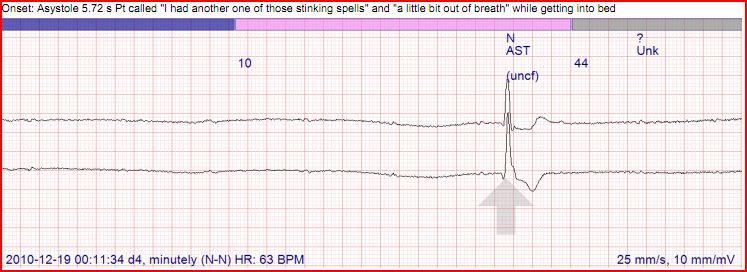
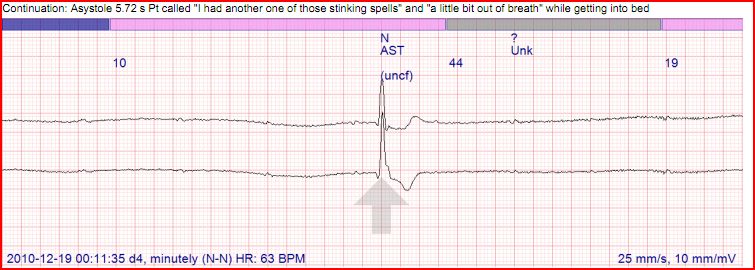
Ah, does this patient have a pulse?
Yes. Patient shortly after this called in to report having a "stinking spell". Could not get any specifics other than that from the patient per the supervisor that took the call.
-
Hey ya'll. Its been too long since I've been on here. Been going to school and working in cardiac telemetry. For those who don't know me (which may be a lot of you) I love learning about EKG's, and I realize many people determine them differently. I have a couple teaser rhythms that I will post here occasionally until I get bored or no one responds. But please give these a shot, be civil to others interpretations if you disagree and I will reveal the answer later.
Just some background on this patient. 69 y/o female on a holter for having "spells". The patient's baseline rhythm is Sinus with a First Degree AV block with IVCD (intraventricular conduction delay). Unknown if the patient has a history of bundle branch block. Thats one of the disadvantages to holter rhythm analysis. So if you want to assume there is one, I wont hold it against you unless you call it a right or left bundle branch block. Identities have been of course withheld for protection of the cardiac offenders (due to HIPAA). There are 3 strips I saved. the first three ( assuming it puts them in the order I uploaded them in) are a continuous strip encompasing a total of 18 seconds. I would have put another one up but it seems I have exceeded the bandwidth. I will try and add it shortly as a comment if possible. (It's been a while)
The program being used is called Pocket ECG. Enjoy

The 4th strip is too large for me to post. If you would like the last strip email me at wrmedic82@yahoo.com.
Thanks



-
If following protocol results in 'suspicious circumstances surrounding death', isn't that pretty much the same as saying, "Yeah, we killed the old bird."?
Since you are the cause of the 'suspicious circumstances' surrounding the death of this woman, (and you've essentially admitted to being the cause), aren't you setting yourself up for criminal prosecution as well as setting the company up for civil liability?
As far as not applying a monitor, I'm just as confused as everybody else. How can you even begin to think you're geting a 'clear picture' of what's going on with the patient if you don't use the diagnostic tools at hand?
In reference to the post where the patient had a valid DNR and said "Help me!", I have to agree, that simple statement completely negates the DNR, even if the ink on it isn't dry.
I doubt this would be a subject to criminal prosecution on the basis that the provider not only did what was felt to be best for the Pt, but also as indicated for the situation by protocol and accepted ACLS algorithm . Although it may have caused the arrest, if nothing was done it could be argued she would have died anyway. Who knows what underlying cause of her SVT was? Epidural head bleed maybe?
I can see how not placing the monitor on the Pt adopts the "ignorance is bliss" notion for DNR pt's, however I would look into your states laws on OOH DNR's before putting this into your medical practice. As stated earlier in Texas (where I live) it only states we cannot do CPR, Shock (defibrillation, pace, cardioversion) or perform advanced airway. Says nothing about monitoring. Everywhere is different.Besides I personally wouldn't want to say "I dont know" to a doc or a nurse if I could have taken the time ahead to find out everything I could about the Pt before handing over care.
Just a side note to my two cents, remember there is two of you on a truck. You can pull over and utilize that person to do CPR or contact med control. Dont handicap yourself. Half @#! CPR is as good as no CPR.
-
In this situation you have to be realistic. What you now have is a couple things that are not on your side.
1. Time
2. Lack of usable resources
3. Distance from nearby civilization
4. Loss of communication
5. Lack of knowledge of the mechanism of the blast (accidental or intentional)
If you are still alive after the nuclear flash and the shock wave that soon follows. You will now have to think survival. Nuclear fall out will begin to occur shortly so trying to go on foot will be futile. Even if you make it to the foothills as suggested earlier, the problem is shielding from gamma rays. Sheltering in place may also be just as futile with central air conditioners, as well as wood-framed houses. Wood-framed houses may hold up, but will not protect from gamma radiation from nuclear fall out. The best protection would be to find a steel frame construction building, preferable with a cement basement, and get to the lowest level as possible. Avoid walls and windows that could expose you to gamma radiation.
Communication at ground zero will be limited to the range of your voice. It will be a prayer if you can communicate to someone on the outside. Although there are things to protect devices from EMP, (http://www.afcea.org/signal/documents/LEA.pdf) It may not be available in a rural setting where code enforcement means that as long as the building doesn't burn, it is considered acceptable.
Your medical resources will be severely taxed, hospitals will not be at your disposal. Triage will be essential in treating patient's effected. Assume all Red patient's will become black, and treat accordingly. This is no longer a situation where you want to save everyone. Otherwise you will save no one. The cards are not stacked in your favor, so you should gear your approach as such.
I know this will not sit well with some of you. Sorry but someone had to say it.
-
Its funny you say that herbie cuz I have talked with 2 ER docs who use the NEXUX for clearing c-spine and love it. Both docs are also medical directors for EMS, and will not allow their medics to clear c-spine using the same technique. It all comes down to liability and how much or little of it do you want.
-
If a paid EMT or Medic refused to take a job, there would be calling for their job. What is the difference?
Thats why we have gloves, gowns, masks and glasses on the bus. Wear them.
Why should the citizens of that community suffer because of her ignorance and ineptitude?
Refusing to enter a shooting scene before PD clears it is one thing.
Refusing to enter a burning structure without the proper gear, training, and team is one thing.
Refusing to go on flu like symptoms call because you have not been vaccinated is completely another.
I wonder how many years prior she got the flu vaccine?


I agree with what everyone is saying here. The problem that I feel is being overlooked is that she is a volunteer. Im not sure how NJ defines duty to act, but where Im from its really a grey area. Just because the department drops a tone for a medical call doesnt mean I have to go. (of course Im gonna go without question) My legal duty to act doesnt come into play until I check en route over the radio. I do both paid and volly work. Personnally she needs to pull her head out her butt, and remember that its the citizens that provide the funding for new equipment, and that she has a direct impact on the PR of her department. If she isnt goint to take care of the citizens she is sworn to protect. If I was living in her district I would be appauled if they asked for additional funding. From a patient care stand point Im not going to allow a guilt cloud over my head cuz a kiddo had flu like symptoms and crashed. (I know that it maybe far fetch).
-
1
-
-
MRX is the philips heartstart manual defibrillator which when combined with the QCPR sensor, gives feedback on compression effectiveness. This pad sits in the middle of the chest where you perform compressions and gives feedback in real time to the Monitor to advise CPR changes *push harder, faster, slower...... wait sounds like a night out with the wife.... anyway back to the topic*
Only downside to QCPR, not compatable with the MRX units with Paddles as it requires the pads to collaborate the resus information as the pads sense the recoil etc.
More information can be found on the philips health care site.
Scotty
They do have a Mrx that can opperate with the pads. They have a doohicky that is commonly nicknamed the hockey puck that sticks to the chest with adhesives so to monitor compression depth, rate, and recoil. I like the phillips monitors myself.
-
Agrees with Spenac's co-workers j/k
I do repetitive questioning every now and then also when it comes to assessment. Its 50% of I forgot (we are human)and 50% I want to see if the patient gives me a consistent answer. Im not going to type my complete rational for this. But I will ask you how many times does your patient tell you one thing and the hospital staff another?
Although this may not prevent the patient from telling another story at the hospital.(especially is the patient has dementia) It makes me feel better. Dependent on the situation, it could be a good assessment tool. Don't worry so much as far as your partners experience. yes she is a wealth of information, but you have been trained with the same skills(assuming your the lead on the truck or have the same level certification). Perfect those skills and you will be fine. Im not saying to dismiss your partners experience totally though. And how have you tried to resolve this issue with your partner? Have you talked to her about this problem? or does she do this in a sense to try to be funny on scene?
-
I don't understand why this topic needs to come up every month or so. It is always the same discussion, and it always ends up the same way.
In my opinion, it boils down to this:
If the patient is alert, oriented, and subjectively capable of making an informed decision, he or she may refuse.
Otherwise, he or she may not refuse.
The sticking point here is always of course in the subjectivity of "informed decision" and "alert and oriented." That is going to have to be a personal, on-the-scene decision that an individual provider makes based on his/her assessment of their unique patient at that particular point in time. There is no broad rule here to answer the question once and for all, which is why it is so frustrating to see this topic come up over and over again. Anyone who says they "never clear drunks" or will "always clear drunks" is either lying or an idiot. The assessment is subjective, and relies on a very simple and basic rule, as noted above.
Fiznat,
The question isnt whether or not we transport. So assume you have come to the conclusion this person aint goin to the hospital. So the question is how are you going to clear the call. Would you have the person/patient sign a AMA refusal, Release at scene and document the contact and that there were no medical complaints, or would you say this is a false call and clear the scene.
Who is responsible for your patient?
in General EMS Discussion
Posted
Legally speaking, you are responsible unless that RN is going to assume care throughout the whole patient care process. (unlikely story). I have seen this first hand on a couple occasions and it has helped, but also has almost come close to biting me in the butt.
It's a judgement call