


hammerpcp
-
Posts
701 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by hammerpcp
-
-
I find myself thinking about the conundrum related to Asys' butt cyst while doing things around the house...weird. Anyway, here's some of my thoughts: Shivering is your bodies attempt to elevate body temperature both in fever states and when the core temp. is sub-homeo. So initially, when you were cold shivering your febrile state just hadn't registered yet on your temperature measuring device (I assume you didn't attempt a core temp measurement which may be more accurate although you might still have been subclinical, in the febrile dept.).
So you had some kind of mysterious infection. At least the cyst is gone.
-
Offhand I am not sure if any actual research has ever been done regarding the actual amount of air required to cause problems when introduced by different routes (venous, arterial). I do know that every time I hear some one talk about it the quantity gets bigger though. It might be interesting to do some searches on that actually.
Regarding the dental drill and risk of air embolism, here are a couple of links after a quick "Googling":
http://www.cja-jca.org/cgi/reprint/37/1/112.pdf
http://www.anesthesia-analgesia.org/cgi/co...tract/106/1/249
http://www.southernmaxillofacial.com/downl...ill-surgery.pdf
http://findarticles.com/p/articles/mi_m0MKX/is_/ai_n11841559
From my reading it doesn't seem to be a big risk. Let me know if you find out anything else about this

-
Interesting case. I learned a new word too. I have always heard this phenomenon referred to as "R on T" (waves).
-
As an interesting side note, this scenario reminds me of something someone told me once regarding the risk of embolism related to drilling in the mouth by the dentist... Cerebral air embolism if I recall correctly. Otherwise I would have a high index of suspicion regarding anesthetics when responding to calls at a dental office.
All death is fundamentally caused by cardiopulmonory arrest

-
lol.... the more things change the more they stay the same. :wink:
-
The point is, are you saying that you routinely give D50 to pregnant women?
If they are hypoglycemic and symptomatic, yes. Why not?
-
Actually this is done in the field all the time. It is another part of the puzzle that you can relay to the hospital. I did not intend to sound all self righteous and condescending. I was taught this as an ECA ( first responder ) and so was very surprised that you were not familiar with it, plus you asked if I was joking for mentioning it. It is a very good predictor of what is going on especially in adults. Like most other prehospital exams it is not all conclusive. It will require confirmation before they start surgery. Another good test is the pinch an inch test.
Really maybe I am in the minority because I believe the more info the better I can treat and the better patient advocate I can be. ( see do you look and touch discussion as well as nut is swollen and hurt thread )
You are contradicting yourself. On one hand you agree that it is an inconclusive test and then in the next sentence you say how useful it is. There are all kinds of stupid useless tests you can do in the field under the guise of obtaining more pt information, as if MORE information equates to BETTER information, which of course it doesn’t.
I take issue with your implication that those that don’t conduct these admittedly inconclusive and therefore useless and time wasting tests, which are therefore more likely NOT in the pts best interest, are somehow less adept health care providers. This is what I meant when I noted your air of condescension. Good pt care occurs when practitioners use clinical judgment to direct them in what tests need to be done and what tests don’t need to be done. Let me make my position dead simple: More information does not equal better information, does not equal better pt care, does not equal better diagnoses, dose not equal faster or more effective treatment.
-
http://www.fda.gov/bbs/topics/NEWS/2008/NEW01788.html
FDA: Chantix's Link to Neuropsychiatric Complications 'Increasingly Likely'
The FDA has issued a public health advisory on Chantix (varenicline), saying, "it appears increasingly likely that there may be an association between Chantix and serious neuropsychiatric symptoms."
The smoking-cessation drug, still under review by the agency, may have additional warnings added to its labeling.
The FDA announcement emphasized the following:
Before starting Chantix, patients should inform their clinicians about any history of psychiatric illness.
Providers, patients, and their families should monitor for mood and behavioral changes during and after Chantix treatment.
On the other hand smoking will kill you or make the life that you do have shit because you can't breath. And Michael did you read the website? Quote: "AVRT is simple, quick, and easy so much so, that it may seem "too good to be true." " No offence but everything they say in the FAQ is pretty much the exact opposite of what I said and believe.
Yes, Buprion aka Wellbutrin aka Zyban are all the same drug. It can cause seizures however the more common side effects are insomnia and increased sex drive. Which med are you going to ask your doc for now?
Admin: your spell check program is almost worse then my natural spelling deficits.
-
Yea, I'm sorry here, but patient protection comes before any "rights" you have to free practice of your faith. If you don't want to bare your arms, then go work in psych or podiatry.
Or the US or Canada.
Where did you find this article may I ask? The editor was having a nap when this one came across his/her desk evidently. It doesn't lend a whole lot of credibility to the article or publishing organization.
-
Here ya go, Boss. Just plug in "smoking" where any addiction is mentioned.
:roll:
Sorry Mike, but not with you on this one. When you are done with this website be sure to give your house, your children and any income you will earn in your life to the nearest religious organization.
Quitting smoking is hard. It takes the average individual seven attempts to be successful. That means that many people take more then that to finally get over the addiction. I have no idea what Chantix is but I suggest that you use any help you can get. We have a drug called Zyban (Buprion) which may or may not be the same thing???
Every time you try to quit you will learn more strategies on how to stay quit. Each attempt is not a failure but part of the learning process. There are many websites out there that will offer you suggestions on how to quit. They are mostly helpful, but of course lifestyle change is always difficult to implement because it isn't easy and we are all looking for the easy way. Start exercising.....you will notice how SOB you are. Believe that it doesn’t have to be this way. You can feel good when you exert yourself. Also, it minimizes wt gain and gives you some uplifting brain chemicals. Love yourself, your body. Treat yourself like a child that needs caring for...feed it the right foods....make it exercise even if it doesn’t feel like it...do the laundry when it needs to be done and clean the house....your environment has an amazing effect on your psychological state. And know that you are worth living in a nice and clean environment. Don't smoke indoors. It's nasty. its dirty you stink and you never get away from the unhealthy atmosphere- also your kids or pets or roommates don't deserve to be slowly killed by your self destructive indulgence.
And if none of this convinces you know that you WILL die a horrible death. You will be unable to catch your breath...you will be panicked and as scared as you have ever been in your life...you will slowly suffocate and you will know that you made a decision, many many decisions in your life that brought this state upon yourself...and no one will be able to help you.
I recommend the patch. 8)
Don't waste your time on that hypnosis crap either. A good rule to go by is that if it appears to good-to-be-true it is. There is no 'easy' way.
-
LMAO at "ensure pt is in secure location".
I have a mental image of getting Pt's to stand at the top of a long stair case prior to Adenosine admin.
(AZCEP Is right about the sinus tach thing)
Adenosine has a nasty habit of causing sudden death in pt's who are in Atrial Fib w RVR. So make sure the rhythm is regular!
I had a pt who i suspected to be in an SVT, however the QRS complexes were wide. I thought this was due to a BBB..........the Dr rather than take a chance on Adenosine (althought the half life is so short it is relatively safe) he administered Amiodarone which is useful in both ventricular and superventricular tachicardias. Just a little tidbit for ya'll.
-
I don't have cable and I don't ever watch American TV so I have no idea what drug you are referring to. Glucagon is used to relax the esophagus when there is an obstruction there (for example a quarter).

I don't think the mechanism of action is actually known. But it sounds like your Dr suspected you were experiencing reflux causing laryngospasm potentially? And therefore tried you out on glucagon which actually did the trick. Who knew? Also I think the usual dose is 1-2mg not 0.5mg, so maybe he was just experimenting on you.
-
Man we keep disagreeing. If I have a female bleeding excessively or bleeding when not her period, she gets checked. I need to see what is happening to provide proper report and treatment. What color the blood is. Whether thick, clotted or thin. Perhaps she is miscarrying even when she doesn't know shes pregnant. I may open the labia in order to inspect for sores, etc. So much can be noted with a hands an eyes on approach.
You're right we do disagree. I don't know what your training is but that is so far out of my level of expertise as an advanced care paramedic I wouldn’t go near it. I also think you would be completely in the wrong if you did. We are talking about a stable patient in no to little distress who is completely capable of describing her symptoms to you, and you are performing a pelvic exam with no training, no experience, and really no idea what you are looking for or even what anything means if you do find it?
What does your medical director have to say about your approach?
-
Julian, Narcan had always worked with me whether it was hydrochlorate (a mickey) or Rohypnol. I never had Narcan fail in the field, along with the D50.
Why would you give narcan for Rohypnol? I wouldnt expect it to have any effect seeing as it is an opiod antagonist.
EDIT: I forgot to say anything about the pt. Why does he have water on the brain? Is he perhaps an alcoholic? Maybe a little thiamine and dextrose will do him some good.
-
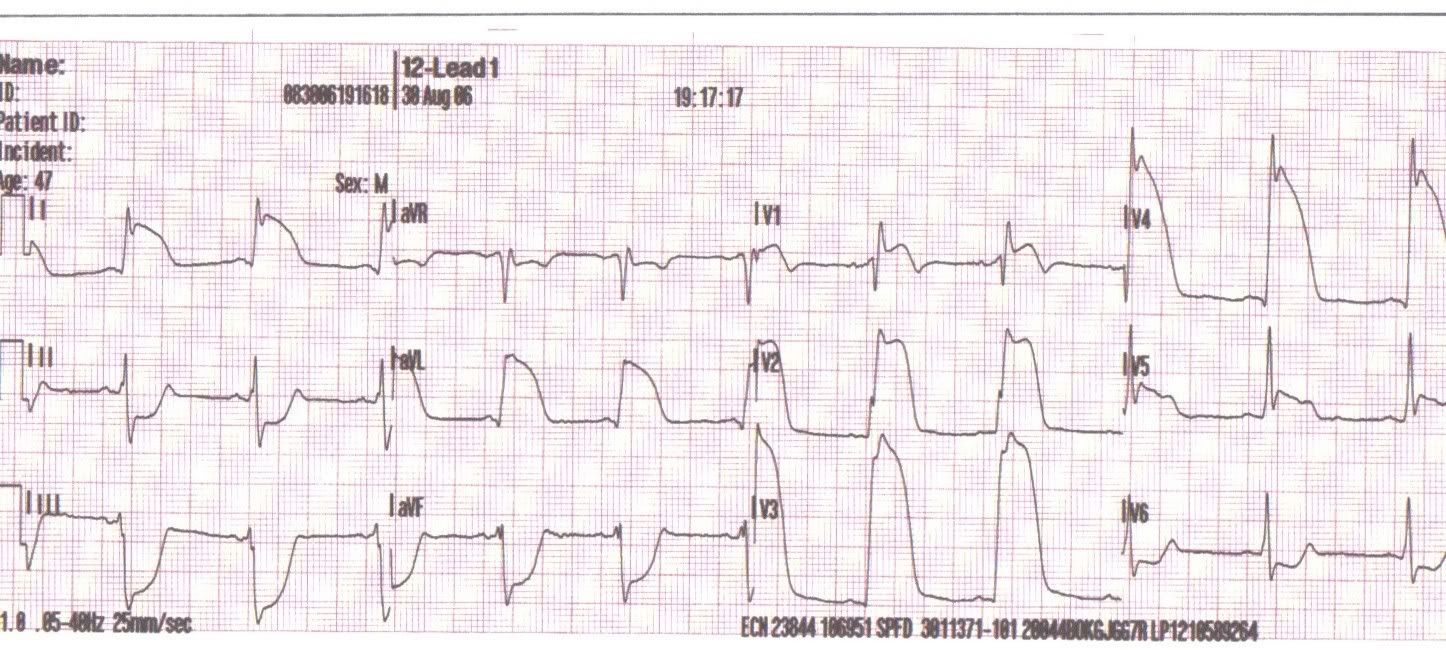
47 year old male, found on the bed. States he was mowing the lawn when he developed severe substernal chest pain. No radiation of pain, mild shortness of breath. Wife called 911 less than 5 minutes from onset of symptoms. Our arrival less than 6 minutes from call.
12-lead performed within 2 minutes of patient contact, rapidly moved to ambulance, thanks to the fire department cooperating. Scene time less than 8 minutes. (They're always in the back room of the house.) Less than 10 minute transport to ER. Treatment included: 18 g IV x2, ASA 162 mg PO, NTG x2, high flow O2, Morphine 10 mg IVP, Zofran 4 mg IVP, NTG drip established and titrated to 50 mcg/min by arrival to ER. Unable to transmit ECG, however called ER en route with patient report. Onset to cath lab, less than 40 minutes.
The patient's wife caught us outside the ER a day or so following this call. She told us her husband had gotten 3 stents during cath and would be coming home in a few days.
Everything came together for this patient. Quick access by his wife undoubtedly saved his life. The fire department were invaluable removing this man from his dwelling. I happened to be working for a hospital based EMS service and transported to my hospital. The ER staff know all of us, and trust all of us. This call will always be the best call I'll ever run.
Question: Why did you administer an antiemetic to this pt? Was he (she?) vomiting or was it prophylactic?
Sounds like a good call. Good work.
Also, Theotherphil it sounds like you really saved that guys life, no doubts abut it. Congrats man. -
Are you hooked for life or can you stop using it and revert to not using it, maybe by administering an antidote/repellent?
There is now also a useful RainX antagonist which can be self administered internasaly. It is not a long term solution but it is an effective stop gap measure to reduce the over all harm done by RainX abuse.
-
There are no absolutes in medicine. Although it is fun to illicit a reaction by speaking in extremes on this forum I concede that in reality sometimes it IS appropriate to examine the genital. However, it is not ALWAYS appropriate. Many folks (read: men) are sick and desperate and would love for a paramedic- or anyone really- to handle their goodies, and thus are not beyond malingering to achieve this goal. Besides the issue of illegitimate complaints there are also several legitimate complaints involving the genitals or perineum that don't necessarily require an exam either. Vaginal bleeding for example. If the pt is not in any distress and has stable vital signs and can describe to me how much blood has been lost and over what period of time, there is no reason for me to take a look. (Unless I am suspicious that there may be babies head sticking out I guess)
As far as the medical "team" goes.....I am skeptical that this even exists. Even when I do a full exam, and have a working diagnoses based on my findings, the fact remains that the hospital staff rarely even take what I have to say into consideration.....and that's if they listen to me at all. Perhaps that is just the situation here, but I doubt it. Also, pts are almost never sent to the waiting area if they are brought in by ambulance. Hence hours and hours of off load delays. So, to argue that taking a look at big Stevo's urinary catheter and palpating his testicles because he has had a little discharge lately is going to speed up his care is completely false. I think I have had my say on this. I am not a bad medic for making a judgment call on what assessments are necessary and appropriate for a particular pt and which ones aren't. You do the same thing every day.
-
Many things can lead us to suspect torsion; however, the physical exam can provide evidence to support our theory or provide evidence to disprove our theory.
For example, a prepubescent male complains sharp and intense scrotal pain. This information alone would lead us to suspect torsion. However, during the exam we appreciate a small hair follicle scrotal abscess. This changes the entire course of treatment and urgency of the patients condition.
While you could argue that this does not directly effect your care, it in fact does. You fail to perform the assessment and provide the ER with an incomplete picture. The patient ends up filling a bed that should have been filled by a patient experiencing an emergency. It is difficult for some of us to appreciate; however, the assessments and decisions initiated in the field do ultimately effect the disposition of our patient and other patients. We must look beyond our little box and realize that we are part of a much larger picture.
In addition, we can appreciate problems such as phimosis, para-phimosis, penile fracture, and priapism with a physical exam. All of the following problems require urgent treatment and your field assessment of the findings can help these patients receive the care they require.
Take care,
chbare.
Many of my pt's experience priapism when I examine their genitals.
Don't get me wrong I appreciate a good prapism as much as the next guy, but there was no information I could not have obtained just by asking the fellow. And when was the last time you had an ingrown hair present like testicular torsion with or without exam? Puhlease.
As far as the pt getting better care in the hospital, that is pretty much the murses and moctors job isn't it.
-
Are you joking? You have never performed heel strike or heel tap or markle sign , just some of the names for this test?
This is an old pretty reliable exam to help determine if it is appendicitis.
http://or-live.mediwire.com/main/Default.a...rticleID=118602
http://books.google.com/books?id=fs6sQlM0z...BbptM#PPA176,M1
http://answers.yahoo.com/question/index?qi...22174621AAtOZU2
I have never heard of this test before....and before you get all self righteous and condescending let me remind you that I am in pre-hospital emergency care and this test is obviously not something one would generally do in the field.
Upon investigation this test isn't even conclusive. Also, a bump in the road may prove just as useful as taping the heels in locating the pain.
-
Do you have to examin the testicles to suspect testicular torsion? How about vag prolapse?
-
chbare
Excellent response. I can not understand why so many are afraid to do their job. Trust me I have no desire to grab a guys nuts, but if thats where his complaint is I need the info to pass along to the doctor. Perhaps as chbare mentioned my actions just might get them definitive care faster.
If you are afraid to touch you really need to get past that fear or else look for a new job.
I absolutely disagree with you both. It is NOT part of my job. It will have no benefit to the pt. Period. Absolutely non productive and inappropriate.
-
Well..........the brown one is......
-
Off the top of my head I'm going to guess laryngospasm.
I dealt with this a few months ago. Throat felt tight, I was starved for air, heart rate up into the 140s. It was the strangest thing because I could feel my lungs filling, I knew for a fact that when they put a pulse ox on me it would read high 90s at least, but still felt like I was suffocating. I controlled my breathing, so no hyperventilation.
It would last about two minutes or so...scared the bejeezus out of me! Then I'd be fine for a few minutes, and then it would repeat.
0.5mg of glucagon at the ER and it soon resolved.
Dwayne
Glucagon eh? Interesting. Did they figure out what caused your laryngospasm? Was it idiopathic or what?
-
I still hate my job.
Do you need critical calls to enjoy your work?
in General EMS Discussion
Posted
I do. I didn't get into this field to be a glorified taxi. I didn't invest time. energy and money into training to not use the skills and knowledge. That being said, I am not looking for all action all the time either.