


P_Instructor
-
Posts
416 -
Joined
-
Last visited
-
Days Won
4
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by P_Instructor
-
-
Welcome back. I've got two nephews at U of Tulsa. If you are near there, keep them safe.
-
Another version of the original poster's formula can be used if you are having trouble figuring out weight in kilo's. Just ask the patient's weight. Using the same concentration of dopamine, and only for dose of 5mcgs/min, take the weight and then subtract 2 from the tens column. This will give you a very close drip rate for 5 mcgs.
Example: Patient states weighs 240 pounds. With the 24, subtract 2 making it 22. This is what you set your drip rate (60gtt set) to, 22 gtts a minute.
-
His statement may be true to some, but what about all the first lady's? I would agree to Jackie, but I guess my next choice would be Ellen Lewis Herndon Arthur. Only my preference.
-
How I believe the system works is that there is a range that is considered as a competent level. Questions are asked initially in the middle of this range. If you answer the question right, the next question will be slightly more difficult. If you answer the question right, again more difficult for the next one. If you answer that question wrong, the next question will be slightly easier in difficulty. It is like a waveform when answering. Treat this like a patients pH range, 4.35-4.45. The middle is 4.0. If you continue to maintain in the range of 4.35-4.45 throughout the exam, you will be successful. If you are below the minimum, then you will be unsuccessful. The test could range anywhere from 70 to 150 questions dependant on where you maintain in that range. If you continually fall below the minimum of the range, the test could shut off at 70 questions and basically states that you do not know your stuff. On the other side, if you continually maintain in the upper or above range, the test may shut down because its like beating a dead horse, you know your stuff. The kicker is that you will not know either way until the results are in. If you continue to stay right in the middle of the range, the test may be the full compliment of questions, and you could still pass or fail.
Lot of junk to take in, but this is how I think it works.
PS: they also include questions that are not counted toward your grade but are possible future pool questions. However, you do not know which questions these are.
Good luck.
-
All we offer is an associates degree.....sorry.
-
Apprehension is a good thing as this seems to prepare you for anything that may happen. The problem is that you can never predict what will happen next......so......use the apprehension and 'being somewhat scared' to your advantage. Wanting to get yourself involved, whether being scared or not only increases the likelihood that you are focused to what needs to be accomplished. I agree that your fellow student is a douche and needs to look for a different job. You, with your statement, shows a caring and compassionate emergency medical provider that is there not only for the patient, but for family members also. The aspect of the nurses talking about their weekend plans shows a stagnate persona of individuals that have been seeing way to much death in their job. I guarantee that if that was one of their family members, none of that talk would come into play.
Your feelings are direct on, and you will do fine. Keep your morals and ethics on line and show the others how it is supposed to be done.
Hey give your fellow break the ribs I'm cool student my phone number 1-800-boot to the head and he and I can chat. I'm sure he's an idiot but I'll let him disprove it.
Shucks.....you beat me to the 'punch'!
-
No dude, you dont have to drop out of college to do EMS, in fact, you dont even have to go to college at all.
Kid, get some edeucation behind you, toss your scanner in the bin, get a degree and come back in 3 or 4 years and then you can call yourself professionala
Great comeback Bushmaster. I agree with what you said, and also believe that todays young student need much more basic training before they even think of pursuing the 'professional' EMS career.
-
PMike, I agree with you but also state you may be a little to critical. I am one of those educators (Master Degree in Education) who instruct Paramedic classes. But there are also many non-educators that are very good in the education of students. All EMS educators, in my opinion, should go thru the NAEMSE Instructor course as a minimum. Another belief is that if you instruct, you should also work in the business also (me, still working part-time at least 36 hours a pay period while educating full time).
-
Crotchity - I think Bushy said it.......man, you keep coming up with this philosophy jargon and the hits will be down to zero
Crotchity - I think Bushy said it.......man, you keep coming up with this philosophy jargon and the hits will be down to zero
-
The military service medics provide what is needed for that environment. There is always things that can be utilized from other training that can apply to any situation. Many milamedics can perform tasks that paramedics are not allowed, and that knowledge and skill is very useful. I do believe that the milameds can also take much experience from the public sector into the military and make it work. They, like us, always strive to 'be the best'.
Sidebar: I have a former (recent) milamed (basic level) in my P class that really knows the base knowledge of EMS, and has the military drive and to be very successful as a street medic. He wants to learn, and has a vast amount of knowledge that the military training could be useful in the street sector.
I think it is very interesting. Thanks for the link.
P
-
Welcome to the city. I've been off for a while and when started to read your post, was very glad PMike had you clarify what you meant by knowledge statement. Take the knowledge in, and continually hone it as you will never know enough in this profession.
-
Ruff,
I know what you are going thru. My paramedic class partner, working partner, and great friend also was killed in Lifenet helo crash in Norfolk, Nebraska back in June, 2002. The worst part of this was that day I was dispatching our Medic units and the local helo when I got a call from Lifenet to take a flight for them. I was dumbfounded as I knew they were already enroute to that location. With inquiry, they stated there helo went down. Unfortunately, I had the work schedule right in front of me as my friend also remained in a part time status for our service. We have quite a few of our medics working for Lifenet and when I found out my friend was on duty that day, my heart sunk.
Hang in there partner.
-
Did you check to see if the NAEMSE course would suffice for the instructor in your state?
-
What is the size of your patient (ie. weight, frail, thin, etc...) All things need to be looked at and everyone has good ideas. Any history of prior lung problems that may indicate a small spontaneous pneumo that cannot be detected with lung auscultation??? Just wondering...
-
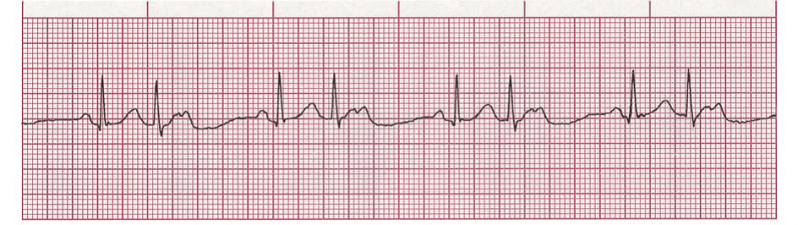
Ruff.......Are those Osborne wave's I see after the 1st, and 7th QRS's?

Oh crap....sorry from the bottom of my heart......just realized you wanted this for students. My apologies.
-
I disagree, I see a QRS for each P wave.
There are P waves in the T waves. Accelerated 2nd degree Mobitz Type II (Classical). There are more P's than QRS's. Regularly irregular......
-
Quick look makes me think of a Mobitz Type II.
-
Welcome.
You do realize you're going to be called Amber from here on out, right?
You didn't know that Amber is the southern Okie slang for Curt????????

-
There are many questions that one does need to consider. How long has this been going on, maybe between these two, whatever. The little puke got what he deserved as the initiator of this bullying event. I do give support to the larger kid who had restraint from pummeling the puke after the first punch to the head. My opinion is that yes, if the bigger kid punched the little one, more damage could have been done. True, a lot of damage could have been done with the body slam, but I still think restraint was used. Pisses me off that another 'big kid' stepped in after the little one got crunched, but realized that he had better not do anything. More support to the bullied kid as he walked away from the situation. I think the point was made. School policies on suspension for aggressive behavior differ from one area to another. Do I believe the larger kid should be suspended, no, but yet one must realize that he should have just walked away and reported the event.
I still give him kudos for putting the little puke in his place.
By the way, I was a skinny kid who got picked on through school, and eventually did defend myself which suprized my attacker. Haven't had any problems since that time with him and remain friends today.......many, many, years later.
-
I disagree, you have noted that this has been an ongoing issue for awhile, so I suggest you go meet with him. That is the adult thing to do. I would much rather someone confront me with an issue so that I can explain myself to them, versus having a long standing grudge over non-sense. Another reason to do this is because you said he is an owner in your service area; although you may never care to work with him, owners and directors usually meet quite often, and they do discuss who should not be hired (informally), as it is almost impossible to get a true "reference" from an employer anymore. He could be spreading the word right now, "don't hire promedemt, he will blast you on facebook everytime he gets upset". Clear the air, you never know you might make a new friend.
"Crotchitymedic would like to go ahead and issue a pre-apology for all those who will be offended by this post"
I have to agree with with you on this one. Get is done 'face to face' and clear the air. It is probably some petty little thing that has snowballed out of control. He may still 'spread the word' but at least the OP would show some maturity in trying to deal with the situation.
-
... with an IFT company so at this point I don't really consider myself a "real" EMT.
Hey Disgruntled, welcome to the site. First thing, don't be disgruntled.....ha.....and you need to realize that all of us have been through the ranks from EMT to Paramedic. Whether your running the 911 or the IFT's, it doesn't matter. You are an EMT. Emergency blood, guts, gore.....hair, eyeballs, and teeth calls are at a very low percentage of calls encountered. Most are the transfer type.
In my opinion, taking transfers and talking with your elderly patient who has seen it all is very rewarding. Some of my best calls were 2 hour transfers with WWII vets (I'm a WWII history buff). This made the transfer seem like 15 minutes.
Being able to talk with a patient even on IFT's is an art that many people have lost.....so hang in there. Look forward to more questions and posts.
-
you never answered my question honestly, how long were you on the scene ? What diagnostic tools did you use to ensure the patient was stable enough to be left at home. If the same patient presented to the ER, would an ER doctor release her based on those same simple diagnostic tools you used, or would the doc order some labs and xrays/scans.
I was just chiding you anyhow.........to answer your question, full physical and mental exam, stroke screen, EKG, reassessments, questioning, talking with the son from out of state, the friend, entire history (which was limited as she hasn't seen a physician for some time, is on no meds, etc.), talking with DHS........all lasting approximately 45 minutes on scene. As for the latter question, I have yet to see an ER doc not do some type of test whether they agree with you or not. I am sure that blood work would have been done at a minimum. When we left after full explanation of our concerns, she was fully aware of the situation and still refused. This was one of those situations where she did not want to go and knew what she was talking about.
Again, the premise for the post was to see if any other instructors actually create scenarios that are similar to this depicting geriatrics/morals/ethics, etc. I do, but again was wondering about others, so I could scratch their brains for more scenarios.
Later...........
-
Read up on brain injury from ground level falls for the elderly before you leave another at home.
Let's discuss the issue presented in my original post. Are you an instructor, and do you instruct in great depth your classes, whether EMT or Paramedic, the geriatric model concerning morals/ethics/ and legal situations? Do you routinely give various examples, situations, and scenarios concerning the same?
Trust me or not, I know what is happening or what can happen with the 'ground level falls in elderly'. After a full assessment, both trauma and medical, neurological and cardiovascular, decisions were made and based upon my knowledge and experiences. I will not just 'take em' for the sake of getting the dollar for the company. Taking someone against their wishes when they are fully cognitive can and will create more of a problem down the road. The patient has rights whether 20 years old or 200 years old if they can make their own decisions with sane mind.
Here is a decent course for you: http://www.gemssite.com/
Otherwise, you might want to review and take this: http://paramedic.emszone.com/caroline/onlineChapterPretests.cfm?chapter=4&step=2
Don't take this as a bash, but a sensitive view on many geriatric calls that any EMS provider may, and will probably encounter.
-
This employee has again shown that high moral standards and professionalism are completely lacking in her world. Let's hope that this time, she is terminated, and no one else hires her.
Terminate. As an off thread (I think there are some), did or does the FDNY actually perform background checks and/or psychological testing prior to employment on the EMS side? Most FD's do, but just wondering on the EMS side.......even though I know some go 'bad' at times...
Paramedic student in need of some help
in Education and Training
Posted
Probably the biggest hurdle to overcome is being prepared for everything. The trouble is that you usually will get calls that you never had enough training for. Having an understanding and being able to employ the cognitive and psychomotor aspect of pre-hospital emergency medical care will always be of best help to you. Never get in the 'tunnel vision' rut and always think outside the box. Use your gut instincts that develop with your experiences. If at least, identify, adapt, and overcome the best way you can.
First and foremost, make sure you develop a sound patient rapport module. A caring voice, gentle touch, and calm demeanor may be the best medicine you can use.