


daedalus
-
Posts
65 -
Joined
-
Last visited
-
Days Won
1
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by daedalus
-
-
Hello,
Thank you for a well presented scenario.
This fellow has a long standing history of fatigue that has worsen over the past six months. The most notable recent changes are:
• Elevated JVD
• Icterus
• Edemous feet
• SOBOE
• Massive Mummur
• Bleeding of the gums
• Bruises
• Hepatojugular reflux
Add to this clubbing. This means this fellow has had a long standing tissue hypoxia.
Now, this is my weak area so bear with me here. I have very little experience with CV Surgical ICU type of stuff. To me is it sounds like a long standing valve issues that has worsened.
As opposed to liver failure causing the fluid over load that has stress his incompetent valves. I have seen a few non-alcoholic liver failure patients present like this (NASH). But, none had a long standing history of fatigue, clubbing and weakness. Most had decreased LOC due to ammonia levels.
So....time to make a Dx.
What is the immediate field diagnosis?
Since the physical finding lean towards righted sided diastolic failure I am going to go with an incompetent tricuspid or pulmonary valve.
What is the underlying pathology and what is the pathogenesis of the recent decline in his condition?
The pathogenesis could be worsening of a murmur he has had all his life. The right sided failure is causing hepatic congestion and the signs of liver failure.
What is the field treatment, and what is the definitive treatment?
Field treatment should be supportive care. IV, O2 and VS.
Definitive treatment will depend. In the ED this fellow would get CBC, INR, PTT, LFT to start. HIV and HEP serology. Ammonia level. ABG. A CXR and a quick look with an ultra sound. The EP would call Internal Medicine to sort it out.
Prognosis?
Good. I have seen bigger wrecks walk out the hospital. Also, he is young without a bad medical history or bad habits.
Cheers
Thanks for your thought out reply!
The CBC will show marked erythrocytosis. HIV and HEP are negative. I could not find the INR, PTT, and LFT, I am sorry. pCO2 is 34 and pO2 is 70. CXR shows cardiomegaly, and dilated main pulmonary artery, increased hilar vascular markings. Quick look on the ultrasound reveals no effusion.
The location of the murmur (LLSB), the cyanosis, the low room air O2 sats, the RV heave, the EKG findings, and the findings consistent with pulmonary hypertension on CXR should help refine your Dx.
-
Here is a scenario meant to expose providers to a patient population that is given no coverage in most of EMS education.
You respond to the park in a poor area of town for a 20 year old Brazilian male with shortness of breath.
HPI: Patient was playing basketball with family while at a picnic, when he became so short of breath he had to immediately stop playing. Sitting down and relaxing did not palliate the sensation and family requested EMS. He tells you that he has experienced mild short of breath for the past 6 months or so and has found that sometimes he is breathing fast even after simply walking to his house from his car. He has been hoping that he had a chest cold or allergies and that it would go away by itself. However, today it is much worse and he is worried. Mother on scene says patient has never been athletic and always tired easily which has always been chocked up as just not athletic, however she has noticed a decline in his condition the past half year. He has not seen a physician because of socioeconomic reasons, and has never really had a primary care physician.
Prior medical history: None. Patient does not see a physician.
Prior surgical history: None
Allergies: None
Medications: no prescription or OTC/vitamins/supplements taken.
Family history: diabetes and hypertension on the father's side
Social history: Born in Brazil at home, and immigrated to the United States 8 years ago. He and his family are impoverished, and the patient works at a local car body repair shop at the front desk. He does not drink or smoke, and lives with family in a house.
Review of systems: General: no fever. decreased exercise tolerance past six months. Patient is easily fatigued. HEENT: gums bleed easily when brushing teeth. slight yellow discoloration of sclera. Otherwise unremarkable. Cardio: patient states that he has had to keep his shoelaces untied because his ankles have swelled recently. Pulmonary: shortness of breath on exertion and very occasionally at rest. no fever, night sweats, cough. no asthma or wheezing GI: occasional dull pain in the RUQ. otherwise unremarkable.
physical.
Vitals: radial pulse: 100 bpm and regular. BP 130/84. resp rate 24, adequate depth. temp 98.8 F.
HEENT: Jaundiced and slightly blood injected sclera is noted. bilateral jugular venous pressure is elevated to cause obvious distention as 45 degrees. some cyanosis noted around the lips.
Pulm: Lungs are clear to auscultation. Chest is symmetrical and atraumatic. No scars noted
CV: A palpable right ventricular heave and thrill are felt at the left sternal border. A grade II-III holosystolic murmur, slightly harsh, is heard at the left lower sternal border. All peripheral pulses are easily palpated and are adequate.
GI: liver span is consistent with hepatomegaly by percussion and scratch test.
Extremities: Finger clubbing is noted, along with slight peripheral cyanosis. some pitting edema is noted at the ankles. Patient has several bruises on his legs, says he is bruising easily.
Your EKG monitor shows sinus tachycardia with no ectopy in lead two. Finger oximetry is 92% on room air.
You can ask for whatever study you would like. I will even give you labs if you ask for specific ones.
What is the immediate field diagnosis? What is the underlying pathology and what is the pathogenesis of the recent decline in his condition? What is the field treatment, and what is the definitive treatment? Prognosis?
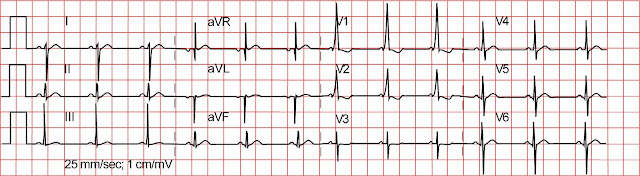
12 lead
-
 1
1
-
-
I've laid out that your view is not the way it is, yet you continue on the tirade. Had my intentions been the way you assume, I'd deserve it. But it's a plain and simple misapprehension of motive.
It is a public forum, knock yourself out. Oh, and by the way, the product uses the word Silly in it's brand title, that's not my words. I'm sure you'll hear about them soon enough, they look like something a child will choke on.
I respect Wendy (ed) for her opinions and I value her knowledge, don't turn it against her. I caused a misunderstanding to occur, something that I apologize for, but won't lose any sleep over. Though, I find myself offended by another user, just slightly, I have thick skin.
"How to piss off emo punks" was the subtitle you gave this thread. I do not see a misunderstanding.
-
1
-
-
Your a real winner...........and to support wendy....please....

I really don't care about online popularity contests. The OP posted something on an internet forum where the public is free to reply and I posted my opinion. I can see that you think that destroying property when not nessecary is trivial. A 110 hour certain class or even a paramedic program does not give one the right to indiscrimatley use those shears in your pocket just because you find the way someone dresses silly. How could what you have written in response to my post been any less intelligent or debate provoking than the thumbs down emoticon you have in their? A "real winner"......
-
- Popular Post
- Popular Post
What the hell are these things the kids are wearing on their wrists? Had one that was wearing at least fifty of these Silly Bands on each arm, in addition to a number of "cause" bracelets. I cut them all off, instantly pissed off. But my first aid for 'emo bandz', is telling them to knot them back together and call them "battle scarred bandz". So, I hereby coin that phrase, but feel free to use it in order to calm them down. HA HA lolz
Your eagerness to cut off clothing which you find trivial because of your intolerance of a certain group of people is disturbing. I have never had to cut off clothing on non critical patients, and kids at a concert are probably not critical patients. Have you never gone through a phase as a teenager? This can be seen as willful distraction of property which is a crime. You have betrayed the trust given to you as an EMS provider to do only what is right for your patients. Looks like once again flashlights, badges, lights and sirens and uniforms have attracted the wrong type of people to EMS who bring the wrong attitude to the job.
Wendy, plus one for a great post.
-
5
-
- Dr. Whitecoat BlogA child was born at 25 weeks gestation – 15 weeks premature – and was not breathing. Babies born at this age have a viability of 50-70%. In other words, up to half of children born at this age of gestation die. The family called 911. The paramedics arrived, performed CPR on the child, and brought the child back to life. I know a lot of physicians who would have difficulty resuscitating such a premature infant.
These paramedics should have been commended as heroes for saving this child's life.
Instead, they were sued and found liable for $10 million.
http://www.epmonthly...ility/#comments
http://connect.jems....c:298459&page=6
As others have said, ambulance services and paramedics will continue to respond to and mitigate medical emergencies until the very people we are called to treat cripple us with frivolous, disgusting lawsuits such as this one. Refuse to transfer a patient to a higher level of care in an emergency, get sued. Transfer the patient to a higher level of care for emergent, necessary, lifesaving and sustaining care, get sued.
-
Sure! You click on apply, fill out all the little information boxes and hit submit. Then you wait for an email or phone call. Then they set up a time to talk to you. Kind of like any other job application process (is that what you meant?)

http://emtlife.com/s...ighlight=Kuwait
No. But thanks for the link.
I am curious to know what to expect on the job, it seems that it is a standard ambulance paramedic gig on a logistics type base in Kuwait. Am I far off on my assessment? Ill be contacting CHS within the next few days for their spiel, but it would be helpful to me if I could get some information from someone actually working in Kuwait, I find it best to get multiple angles on something before committing to it.
-
We are here because some simple self-replicating nucleic acid formed on earth some time ago, and through Darwinian evolution an incredible amount of biodiversity arouse. Our purpose in life should be to maximize well-being and foster a rich, peaceful, and advanced human culture and spread well beyond the earth to ensure our eggs are in more then one basket, in order for survival of the human race. Otherwise our demise is rapidly approaching from human war and religious intolerance, asteroids, a pulsar star destroying the ozone, global warming, climate altering volcanic activity, etc.
-
-
I think the response you got was because you said wrote your previous post in response to people talking about changing the title to progress EMS. You made it seem like you were a little above that because your specific papers already said just "Paramedic". That's not the norm in a lot of places, though...and even EMT programs are still teaching EMT Basic and EMT Paramedic.
The MICP is a joke I've been told (from people who have transferred into the state)...as far as what an MICP really is...
I was speaking about California. The name change has already occurred here, if you take a look at the CA EMSA's website they have changed all mention of EMT-P to Paramedic, including in the Title 22 text of state law. So by law, at least in California, there are no more EMT-Ps. I understand that most of the country still refers to medics as EMT-Ps, and I do not think I am above the possibly large number of great paramedics in these parts of the country. However, I am glad that the NREMT and Cal EMSA have decided to drop the "EMT" from the title, and I hope the rest of the nation will follow in suit. This is not an ego thing, it serves a couple of very important functions including decreasing fragmentation of EMS provider levels, showing that we in EMS are attempting to move past our infancy and become a full fledged allied health profession, being able to provide superior patient care, and giving ourselves a chance to become something other then a stepping stone. You can call me a fierce advocate for the EMS agenda of the future in its entirety, the name changes for provider levels are just a small part. I look forward to EMT classes moving from 110 hours to 190 as a national standard. I look forward to increasing the basic medical science background of paramedics to a "comprehensive and complex" understanding (wording from the NASEMSO). I look forward to the scope of our education and practice to increase to a level where we can function in CCT, primary care, 911, public health roles without going back to school to get a nursing degree. These are just steps in the process.
- JPNever happen short of some sort of drastic adverse event (and I doubt that any adverse event will reach that level because EMS primarily operates at the individual level). What's going to need to happen is either the public demands more or the providers demand more. Organizations like NAEMSP, NAEMT, NASEMSD, or the other alphabet soup EMS organizations are going to have to be the ones to call for higher standards.Which they are starting to do. I have heard from some people close the NREMT and the NASEMSO, the EMS agenda for the future is being taken very seriously. You can expect to see the updated sets of curriculum within the next year or two, with major textbooks coming out next spring for the new provider levels. NREMT will no longer test paramedic candidates who did not complete an accredited program. Small steps that were long overdue, but here they come.
-
Yes, by 2014, it will only list the position as "Paramedic". But since that hasn't happened yet....My point is valid.
http://www.emtcity.c..._1&#entry241887
This is exactly the kind of 'title love' I'm talking about!
You'll notice in the article directly from the NREMT that it clearly states EMT-Paramedic.
I'm not here to quibble about titles, I could really care less. I've got more important things to worry about; like getting my advanced degree so that I can be a better practitioner, and treat my patients to the best of my ability.
While you may not care about titles, I do. Call me shallow, but I see this as a vital step in the advancement of the paramedic profession. No one is going to want to help increase the educational requirements, practice rights, wages, and reimbursement for mere technicians. You say you are concerned with providing the best possible care for your patients, and so am I. We will provide better care for our patients when we purge the "technicians" from the ranks of paramedics and start to become a truly vital, flexible, and educated allied health profession. While the EMT-I to AEMT and EMT-B to EMT changes have not yet occurred, all the documents I have from the National Registry do not include EMT in the paramedic title.
-
What I still don't get is this:
Why are people so hung up on titles? It's not like there's any more glory or praise in a 'superior title'.
Like it or not, according to the NREMT and NHSTA a Paramedic's actual title is NREMT Paramedic or EMT-Paramedic. So essentially a Paramedic IS an EMT.
My NREMT card says "Paramedic" on it under classification, not EMT-Paramedic. My California license says "Paramedic" on it, not EMT-Paramedic. My degree says Paramedic on it, not EMT-Paramedic. I am not a technician. My post-nominal for California is MICP, not EMT-P.
Here is some reading on the name change.
http://www.nasemso.org/EMSEducationImplementationPlanning/Toolkit.asp
-
This thread and previous threads like on Trauma have really shown OUR lack of understanding of the entertainment industry, not their lack of understanding of us. Television and film have a long history of entertaining us by stretching truths and fictionalizing everyday situations. Law and Order does not accurately portray law enforcement or the practice of Law, yet SVU is one of the highest rated shows on television. I have yet to see police unions and organizations taking a stand against Law and Order for showing violations of constitutional rights, excessive force, etc. In fact, the actress who plays Olivia Benson has been honored by Law Enforcement after becoming involved in women's rights and rape crisis counseling. I do not see scientists at Fermilab blasting the SyFy channel for its grossly inaccurate take on particle physics. The American Medical Association is noticeably silent on the TV show House. House portrays physicians as drug addicts with little moral and ethical character, and is grossly inaccurate on how medicine is practiced. Yet somehow the physician community is intelligent enough to understand the entertainment value and realize the public is smarter than extrapolating what they see on TV into real life. The public does not fear doctors breaking into their houses to search for drugs and look through underwear drawers when they are admitted to the hospital. I enjoyed watching Trauma near the end of its last season and saw it slightly mature into a better series in its final few episodes. Like you, I do not preform emergency vascular surgery in the field, but after a long day at school or work, I like to come home and watch something that departs from reality for an hour.
-
2
-
-
talked to the local college, they say as long as I pass the EMT-B registry exam I can be allowed acceptance. So I'll put this other school behind me
Good attitude. Remember, you will get to take the same national test as everyone else after finishing at NCTI. The difference is, NCTI takes a lot more money form you than the local college, and their classes do not apply towards a degree. What you should do is finish your EMT class, enroll in your local community college and take anatomy and physiology and than sign up for paramedic school. If there is a waiting period before you can start the medic classes, taking medical terminology or some of the pharm or patho classes associated with the college's nursing program (if it has one) can only help and make paramedic school easier.
-
Thanks guys for all the input. Santa Barbara County EMS along with AMR in the same area ran a trial for zofran, and California decided to add it to the paramedic scope of practice because of its demonstrated efficacy in the trial. Unfortunately, as far as I can tell, the only county that has decided to bring Zofran on permanently was Santa Barbara itself. Most SoCal EMS systems are pretty resistant to change even if it means bringing on a drug with so few side effects and such potential to help suffering patients in the field.
-
Diphenhydramine (Benadryl) "Antagonizes the effects of histamine at H1-receptor sites." In addition to reducing the net effect of a histamine release this mechanism of action also reduces nausea making Diphenhydramine an effective antiemetic. Like other anti-histamines however Diphenhydramine also causes CNS depression resulting in drowsiness.
Dimenhydrinate (Gravol) is a salt mix including Diphenhydramine and a stimulant (a derivative of Theophylline if I recall correctly). The stimulant in Gravol helps to counteract the CNS depressing effects of Diphenhydramine on its own (Neither does anything until disassociated in the body). Therefore the component of Dimenhydrinate that functions as an antiemetic is exactly the same as the active component of Diphenhydramine.
Zofran has a completely different mechanism of action which I suspect has something to do with why your medical director has chosen it over Diphenhydramine or one of its derivatives.
rock_shoes, I understand the mechanism of both benadryl and zofran, and I understand why zofran is superior to benadryl for n&v. What I am looking for is some evidence of benadryl's antiemetic properties beyond the occasional "diphenhydramine is also a antiemetic" found across the web. I am also looking to see if anyone here has protocols that allow benadryl for nausea in their system.
-
Hi folks. I am finishing up training as a paramedic in a system where we have zofran and liberal indications for giving it on standing orders. This has been wonderful and it is great to be able to see the results for nauseous patients in the field. I may take a job in a system without zofran and am wondering if any of you have standing orders for benadryl as an antiemetic. I cannot seem to find anything on google scholar that would point to its efficacy or lack of therefore for nausea and vomiting. Incidentally I have seen it as a protocol for RNs at a local ER for co-administration with morphine and dilaudid to prevent n&v.
-
"Extend physician like care" makes ambo's sound like a doctor's bitch, hence, being subserviant to the house of medicine!
What about the other 90% of patients who do not have some emergent life threat?
Have you not been listening to me scream for pages now about how we need to get away from proving "life support" and do something about the other 90% of people that all the ambulance can do is take them to the hospital?
Look at ECPs in the UK (dubiously, no press please Professor Malcolm Wollard), CARE/ECP in New South Wales, ECP (urgent community care) here in Wellington, CREMS (community referrals by EMS) in Toronto.
Until EMS gets its thumb out its arse, away from the 10% of jobs that are "exciting" and takes the 90% of its workload which is not glamorous and exciting SERIOUSLY and develops appropriate linkages into the healthcare systems for these patients then I dont think it's going to get very far.
So ... a Paramedic should be defined as at the VERY MINIMUM a "health professional who provides emergent community based health assesment, treatment, referral and transport as appropriate to the to enable them to recieve the most appropriate healthcare for thier needs" or something VERY SIMMILAR
To clear up a few things, I do not mean that the ideal paramedic is just the eyes and ears of a doctor on scene. What I mean by extending physician like care to the field is just that, extending good evidence based medicine into the non clinical environment. I support the idea that Bledose has been pushing recently, that online medical control is a waste of time and has no place in a modern EMS system. Paramedics should not be calling for orders for adenosine only to be told to just bring the patient in. They should have the authority to start their own treatments in the field based on the scope of their education.
-
You need education in the basic medical sciences to synthesize information obtained from a history and physical exam and turn it into a working diagnosis. While an EMT and paramedic might both notice unilateral leg swelling and warmth, only the paramedic will be able to come up with a list of possible pathologies. What about cardiac and lung auscultation? What about a cranial nerve exam?
-
The Paramedic in the US is ideally a professional educated specifically to extend physician-like care to the scene of an accident or emergency. It is our specialty. There is no need to replace experts in out of hospital medicine (paramedics) with doctors or nurses. The need to go to the bachelor of science level is undeniable given our responsibility, and to insulate ourselves from a nursing profession attempt at gaining in on prehospital care (which could easily be done since they have the foundation education to do so). We should also look into making the ambulance the "paramedic's domain". We should take CCT back from the nurses and work on establishing ourselves as the leaders of transport medicine.
Call me idealistic, because I am.
-
So what titles do you suggest we use instead, I have mine above but what do you all think?
I would like to preface my post by giving my support to the changes being made at the national level as we speak. EMT-Basic turns into EMT, EMT-I turns into AEMT, and EMT-Paramedic turns into paramedic. The accompanying changes to education are also a step in the right direction. None of this is perfect, but it is a small step in the right direction.
If I could do whatever I wanted, I would have Emergency Medical Responders and Paramedics. That is it. The EMRs would be firefighters, dual role department (like harbor patrol and life guards), etc. It would closely match the EMT in skill set, with an expanded classroom and clinical time. EMRs could also, with further training, work with a paramedic on a transporting unit. Paramedics would be on transporting units, and could be placed selectively as first responders. Systems would limit the amount of paramedics on shift at any one time so that experience is kept up. There would be no ALS or BLS. There would be medical first response provided by the EMRs who acting within the scope of their education, preform medical care to reduce morbidity and mortality until paramedics arrived. Paramedics would bring emergency department level care to the field (what is practical to bring and supported by evidence.)
-
So here we go again us verse dem. I have to wonder why after countless blogs, posts and forums it is apparent to me that the bls vs als is unwinable. ALS will always FEEL SUPERIOR, and lets be truthful they are more educated. If all of us slimmy, no good,communist, uneducated bad spellars and chicken thievin basics were to advance up to als they would be left with little to complain about and no one to ridicule. So in reference to that 'your welcome' I would hate to leave all the ALS providers melancholy. They might turn on them selves and begin to eat there young.
This is not an us vs them or ALS vs BLS thread. It is a thread discussing the needless use of such labels (als and bls) and the education needed to preform medical procedures that should (and every other profession does) require at least masters degree preparation.
-
1
-
-
Again, this is an issue of education. The principle behind the idea of "BLS before ALS" is solid- you must master the building blocks and basic understanding of what you're working with before you move on to more advanced ideas and practices.
The problem is that our education is not structured correctly. You are given the wrong building blocks at the BLS level and with that a false understanding of medicine. It is MUCH more important to understand the biology of medicine than it is to understand how to use a BVM or apply a LSB. Your patient history is one of your most important assessment tools, and if you don't have the correct understanding to inform how you go about your line of questioning, you're simply muddling around and missing the point.
Anyone can be trained to master the physical skills of medicine... whether it's IV's, intubation, cardiac monitor placement... not everyone has the capacity to figure out how it all fits together at the level which allows you to make sound treatment decisions. I will, however, say that once you master the intellectual part of it you must also master the physical skills... because knowing what's wrong does you no good if you're incapable of performing the right actions to treat it. BUT! Without the correct thinking, all the skills in the world are useless to you.
Wendy
CO EMT-B
Wendy, good post. I do agree that we have got our basics backwards. Why does EMS look at pathophysiology of CHF as an advanced provider topic, while it looks at using a BVM as a basic level provider topic? This makes no sense and it is the other way around in respiratory care, nursing, and medicine. If we truly went to basics before advanced, anatomy and physiology would be required before EMT class.
I may be different than most US paramedics, but I choose not to define my job as a set of procedures I can do, but the knowledge I bring to a patient in the field. Most people seem to think a paramedic is someone who reads 3 lead EKGs, starts IVs, and pushes drugs. I like to think of a paramedic as someone who (hopefully) has some real knowledge of biomedical science and who spent time in various wards of a hospital learning the proper way to deliver children, provide airway control, etc.
-
BLS before ALS
you have to be an emt for a year atleast before you can start to be a medic.good emt skills is what makes a good medic.i dont give a damn if you are ALS is you cant to the basics then you are no good to me.think about how many ALS calls really go down on any given day,where i work(in manahttan) alot of calls get upgraded by the callers because they want an ambulance to get there faster but when you get there its bullshit.
yes ALS is hard,i was in medic school til i got hurt at work and had to drop out but so is emt work.medics need us and we need the medics.alot of places double as bls/als and are usually run by fire and thats the true issue imo. if you are a fire fighter then thats great but the system should be kept seperate.ems should be run by someone who has medical traning and not by a fire fighter.
getting back to which is better,neither is better,its what you know and how you do it.i can start a line,do the leads and push drugs better than some of these medics out here but i have seen als do better immoblization and basic bleeding control better than some of the techs who have been on the job for 20 years.
if you are an medic then you need to keep up your emt skills because all als protocols say BLS interventions first and just because we are on scene there to help you otu doesnt mean have us do all of that because you dont want to.learn the new tricks from your emts as for the techs learn the simple things from the medics like how to spike a bag or how to put the leads on the pt.
ems isnt going to go anywhere if we keep bashing eachother,als saves bls but its bls skills that saves als
BLS before ALS? How about we just give our patients the medical care they require. Putting a patient on oxygen is not a BLS skill, its medical care that is preformed by CNAs all the way up to MDs. Also, what is the obsession with calling medical procedures "skills" instead of "procedures". No one else calls intubation a skill, it is a procedure. Are we in 1st grade again going to motor skills class? And as mentioned by multiple posters above, doing procedures requires education not training.
-
1
-
Shortness of breath
in Education and Training
Posted
Early menopause! Spot on my dear Watson. JK..
Our patient's present pathology is rare in the developed world, however the causative lesion is common but is usually corrected in childhood. If you were able to know somehow, you would find that our patient has had his heart murmur all of his life. In fact, the murmur used to be louder earlier in his life and has recently quieted a bit, with the thrill diminishing as well when his symptoms became worse. However, our patient was born at home and has never had proper medical care. Being in a third world environment in rural Brazil, he never had well child visits with a pediatrician and his pathology was never discovered when it could have been treated.
With a holosystolic murmur at the left lower sternal border, an RV heave, hepatic congestion with other signs of RV failure, and RV hypertrophy on EKG you can infer that the patient's underlying congenital heart defect is an isolated, moderately sized ventricular septal defect. VSD is the most common congenital heart defect, and about 1% of all live babies are born with congenital heart defects. You might also consider tetralogy of fallot, however you could rule that out based on his age (20), because he would probably have died before his second decade of life with untreated tetralogy. Further, our patient has been acyanotic most of his life. A moderately sized untreated VSD would account for the delay in full blown RV failure. With the recent cyanosis and low oxygen saturation, along with the marked right axis deviation on EKG and the dilated pulmonary trunk on CXR, you will find that the untreated VSD has progressed to eisenmenger's syndrome.
For most of his life, the hole in the intraventricular septum has caused a left to right shunt. The larger and more powerful left ventricle forced oxygenated blood through the defect and back into the right ventricle, where it was again pumped into the pulmonary circulation. Over time, the increased pulmonary blood flow caused restrictive changes to his pulmonary arteries which progressed to pulmonary hypertension. The right ventricle had to pump harder and harder to overcome the increased pulmonary vascular resistance, causing RV hypertrophy and eventually failure. The enlarged and now powerful RV reversed the shunt, and now deoxygenated blood was forced through the defect into the LV and pumped into regular circulation causing the cyanosis. Eisenmenger's syndrome is a late complication of untreated VSD where the shunt (left to right) is reversed to become right to left. The pulmonary hypertension is irreversible, and fatal. The erythrocytosis is a compensatory mechanism for the chronic hypoxemia. Jaundice and coagulopathy are secondary to liver dysfunction, caused from the chronic hepatic congestion from the RV failure. His prognosis at this point is actually quite poor, and death will probably occur within a few years even with treatment. Definitive treatment for eisenmengers is a heart-lung transplant, but survival past 5 years after transplant is quite rare.
Why did I write this scenario? You will probably never encounter eisenmenger's syndrome in your career. It is helpful however to understand the late sequelae of untreated VSD, because VSDs are other congenital heart defects are very common. But the point of this thread was to introduce you to a patient population you will start seeing of very soon. A patient population that is rapidly expanding, and one that is new to all of us. Because of the advancements of modern medicine, children with congenital heart defects are now living into adulthood, and this is a very new development. It will not be uncommon for you to care for young adults who had very complicated open heart surgery to cure or palliate congenital heart lesions.
JEMS wrote an absolutely useless, horrible article on congenital heart defects last year. The author went in with the idea that EMTs and paramedics were too stupid to be taught about the physiology and altered physiology of the heart, so instead attempted to broadly classify the many different defects into neat little "cardiodromes" dumbed down so that we could all understand. He royally butchered the whole thing and probably left most readers scratching their heads and turned off of CHD.