


Tom B.
-
Posts
72 -
Joined
-
Last visited
-
Days Won
2
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by Tom B.
-
-
As I explained in a recent interview with EP Lab Digest, the cardiologist who's "right" can generally provide an explanation of "why". Tomas Garcia MD used to remind us at the EKG Club that the most common reason cardiologists fail their 3-part board exam is ECG interpretation!
Tom
These are very good strips; the kind that if you showed them to 10 cardiologists, you would probably get 8 different interpretations. -
The altered mental status has me concerned. I would immediately inspect the head for trauma and consider this a neuro patient until proven otherwise. Neurological truama and/or intracranial pressure can create T wave abnormalities. In addition, the QT interval is considerably prolonged (QTc of about 575). This patient needs a cat scan and blood work.
Tom
-
Actually, the first box in the tachycardia algorithm says:
Assess and support ABCs
Give oxygen
Monitor ECG (identify rhythm), blood pressure, oximetry
Identify and reverse underlying causes
In other words, the Hs and Ts are a higher priority than antiarrhythmics.
Further down the algorithm, for stable wide complex tachycardia, the algorithm says:
Consider expert consultation
That's the first recommendation.
It's worth noting that the ECC guidelines were written for physicians. In other words, it recommends that physicians consider an expert consultation (i.e., a cardiology consult) for stable patients.
I don't believe that paramedics are expected to be automatons that blindly follow protocols. Algorithms, by their very nature, oversimplify complex problems. They are not a substitute for sound clinical judgment.
My Medical Control Physician and Medical Director agree.
Tom
P.S. Congratulations on the save.
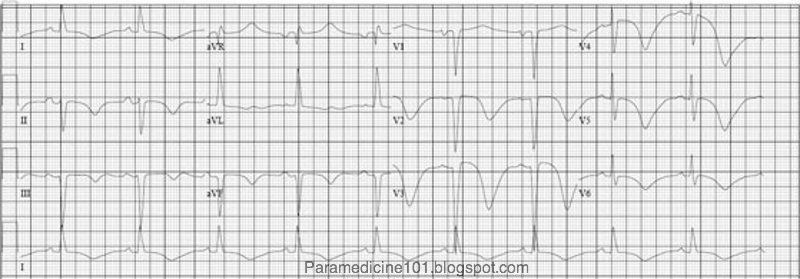
Heh, it's actually post-morbid. This is a ROSC 12 lead from one of my very few code saves. In any case, it is still a wide complex tachycardia. I wouldn't (and didn't) treat this patient with antiarrhythmics either, but I am curious as to your rationale for so universally avoiding medications for these patients. ACLS still says that we should be giving drugs to those that fit in the "stable/symptomatic" category, and those guidelines were produced using the most up to date research available. If you (or anyone else) are going to go off on their own treatment paths, say cardioverting "early" or waiting on the drugs for a patient who remains symptomatic, I wonder what resource you would use to justify your decisions if things went downhill and the fingers start pointing at you. We're not physicians. Right or wrong, we don't get to make up our own treatment modalities.Don't take this the wrong way. I respect your assessment of the rhythm and I understand exactly your academic perspective. Still, shouldn't paramedics stick to the guidelines regardless of how many articles they've read? I think it's a good discussion....
-
fiznat -
Any ECG needs to be interpreted in light of the history and clinical presentation, but based on what I'm seeing with this ECG, I can tell you with 100% certainty that I would not give an antiarrhythmic to this patient.
It's an irregular rhythm, with variations in QRS/T wave morphology. I don't know if the QRS is wide, or the complexes are a bizarre combination of QRS/T. Either way, this looks like a pre-morbid rhythm or a patient who has an underlying metabolic derangement.
I wouldn't rule out acute STEMI or aortic dissection (elevated J points V2-V5) and I've seen acute STEMI create tombstones like we see in leads I, II, aVR, and III. Either way, and regardless of cause, if the patient is hemodynamically stable, then I'm falling back on the theory that "a perfusing rhythm is better than a non-perfusing rhythm or no rhythm at all".
The patient should be worked up in the ED, and the Hs and Ts should be aggressively treated. Once hypoxia, acidosis, electrolyte derangements are treated, and serial ECGs or bedside echo are obtained, a treatment plan can be started that may include a trip to the cath lab.
The last thing this patient needs is a drug like amiodarone, altering the shape of the cardiac action potential and prolonging the QT interval. Assuming this a polymorphic wide complex tachycardia (may or may not be true) I would get an expert consultation prior to treating with any antiarrhythmic (and I would hope the ED physician would do this same). You can't take it out once it's in.
As a final thought, if the patient had an ICD, I would consider the application of a ring magnet to disable tachy functions. We had a similar case a few years ago and the ICD shocked the patient x2 into asystole and the patient was not successfully resuscitated. It turned out to be severe hyperkalemia.
Tom
Another wide complex tachycardia. Would you feel comfortable about "ruling out VT" in this one? Say it was stable/sypmtomatic, which anti arrhythmic would you pick? (and don't give me that crap about cardioverting everyone, that's no fun haha)
By the way, why was this thread moved to scenarios when all of the other "strip teases" remain in the patient care forum? Can we just decide which one they all go in, and leave them there?
-
<s>It's the ghost rhythm. I've not seen it before</s>.
I can see it now!

Tom
81 y/o female with altered mental status.
-
Very cool! Excellent suggestion, fiznat.
Tom
For those of you looking for Strip Tease 9, it's in scenarios thread.I am going to start posting the strip teases simultaneously on here.
The answers will be posted on my blog after a short time as well. I will link directly to it from the post on here.
When you provide your impressions on these posts I ask that use the Insert: SPOILER tool. This is found when you are using the edit screen on the left side under "Quick Access".
Look below to see what it does. Now highlight that black bar.
It looks like this when you use it.
Also, after you provide your interpretation I might ask for an explanation as to how you came up with your interpretation. This will help improve the educational quality of these posts.
To view the strips larger you can usually click on them. If not, try holding the Ctrl key and scrolling your mouse wheel. Or hold Ctrl and tap + or - keys.
Well enjoy, the next strip tease is coming really soon!
-
I've had good luck with Adenocard and Cardizem, too. If "good luck" is defined as terminating AVNRT or slowing the ventricular rate with AF. But what was the point? Looking back on my career (at a time when I had a much different outlook than I do today) I did these things because I could, and because it was fun, and because it meant that I was a "good" or "aggressive" paramedic. It wasn't about the patient. It was about me.
In one of the few (if not the only) studies of prehospital Adenocard, it was given inappropriately 20% of the time, including regular wide complex tachycardia (5%) and irregular wide complex tachycardia (2%).
I myself have seen Adenocard given for patients in acute pumonary edema with sinus tachycardia or AF with RVR. When asked why the paramedic gave Adenocard, they both said, "heart rates > 150 can't be sinus tachycardia".
How many EMS systems educate and train their paramedics to the point where, 100% of the time, a 12 lead ECG is captured with excellent data quality documenting the arrhythmia, the print button is pressed prior to the administration of Adenocard to document the pause, and a 12 lead ECG is captured of the post-conversion rhythm?
In my experience, not many.
As for Cardizem, we recently pulled it off the truck. Why? Because how often do you have a patient with new onset AF with symptom onset < 48 hours who is stable? Not often. And how do you really know for sure that the symptom onset was < 48 hours? Usually when we see AF/RVR it's a heart failure patient with shortness of breath who needs oxygen, NTG, and CPAP. Not Cardizem. Why not allow the physicians at the hospital to risk stratify the patient, do a bedside echo to rule out a clot in the left atrial appendage, and heparinize the patient if necessary? I know some argue that Cardizem won't convert AF. Well, I've seen it many times as a cardiac monitoring tech on a stepdown unit.
So no, I'm not a huge fan of prehospital antiarrhythmics. If the patient is unstable, then cardiovert. If the patient is stable, capture a 12 lead ECG with excellent data quality, start an IV, place the patient on oxygen, place the compo-pads as a precaution, and take the patient to the hospital. Documenting the arrhythmia in 12 leads is the most important thing you can do for the electrophysiologist who follows up on the case.
If you must give an antiarrhythmic, you should do so cautiously, in accordance with your protocols, and with the understanding that any antiarrhythmic can be proarrhythmic, or even fatal if given in the wrong circumstances.
That's why I wouldn't monkey around with AF/WPW in the field, except with electricity, and even then only if the patient was clearly unstable.
Tom
Any antiarrhythmics? I've had some really good luck with both Adenosine and Cardizem. -
The following is straight out of the Bob Page 12-lead book.
Your primary survey of the WCT patient:
1. Measure the QRS width
--- Good idea. If it's not "wide" it's not a WCT.
2. Determine the axis
--- Should be a part of any 12 lead interpretation. Just be aware that axis cannot rule VT in or out. Does a right superior axis favor the dx of VT? Sure. But that should be your default dx anyway.
3. Look at morphology changes
--- Here's where it starts getting dangerous. If you use morphology to "rule in" VT, then great! If you use it to "rule out" VT, then you're living dangerously. This goes for axis and morphology.
4. Look at concordance criteria
--- Same feedback.
5. Look at signs of AV dissociation
--- This is the best evidence that a rhythm is VT, but it's only present 50% of the time, and it's not easy to appreciate on most ECGs.
6. Get a good patient history
--- A history of MI increases the probability that you're dealing with VT, but again, that should be your default diagnosis for a WCT.
7. Do a physical exam
--- Goes without saying.
Wide Complex Tachycardia > 150: Listed by ease of use, Often seen, & Specificity
1. Extreme right axis deviation (ERAD) & positve v1
2. QRS morphology in v1
3. QRS morphology in v6
4. ERAD & negative v1
5. Concordance in v1 through v6
6. RS interval > 100ms any V lead
7. QRS > 140ms if up & > 160ms if down in v1
--- Once again, ruling in VT is fine.
Extreme right axis deviation:
ERAD is also known as right-shoulder axis, northwest axis, intermediate axis or "no man's land". This is an axis > 180 degrees.
--- I've seen it with nonspecific IVCD, RBBB/LPFB, and hyperkalemia. It's not always VT. But again, ruling in VT is fine.
You can determine this simply by looking at leads 1, 2 ,& 3. If leads 1, 2, & 3 are all negative, the patient has ERAD. If v1 is positive with ERAD, the rhythm is ventricular in origin. It is still possible for a ventricular rhythm to present with ERAD and negative v1, this is just lest specific.
QRS Morphology:
1. When you have the "bunny ear" shape in v1. Having the left ear bigger than the right ear indicates VT. This is also referred to as "big mountain/little mountain".
--- Sort of like this case. Ruling in VT is fine.
2. A single peaked upright R wave in v1 is indicative of VT
--- Negative. I've seen it many times with bifascicular block and even atypical RBBB. But ruling in VT is fine.
3. A single peaked upright R wave in v1 with slopped off end
--- What does this mean? We've already listed a monophasic R wave as a rule-in VT criterion.
4. A fat (> 40 ms) R wave in negative QRS in v1
--- A slurred upstroke of the R wave does suggest VT.
5. A notched down stroke of negative QRS in v1
--- This is called "Jospehson's sign" and I've seen it in VT many times.
6. Any predominately negative complex in v6 suggests VT
--- Or paced rhythm, or cardiomyopathy, or nonspecific IVCD.
Concordance:
1. Negative concordance, meaning negative QRS complexes in v1 through v6, indicates VT or LBBB.
--- That would actually be atypical for LBBB, although sometimes there is a persistent S wave in lead V6 with RVH. Regardless, if it indicates VT or LBBB then it's no help, right? It actually is more suggestive of VT, but that should be your default dx anyway.
2. Positive concordance indicates VT or WPW
--- Or RBBB or nonspecific IVCD.
Measurements:
1. Positive QRS in v1 > 140ms
2. Negative QRS in v1 > 160ms
3. RS Interval is highly reliable. From the start of the R wave to the nadir point of the S wave (the bottom point). > 100ms is VT
--- Ruling in VT is fine.
AV Dissociation:
1. Cannon A waves. These are waves of pressure seen shooting up the jugular veins.
2. P waves out of place and isolated
3. Different S1 (first hear sound).
--- Ruling in VT is fine.
Remember, we are trying to rule out VT. This means that if you have any of the criteria without strong conflicting criteria, call it VT.
--- I missed it, Adam. Where are you ruling out VT? All toads are frogs, but not all frogs are toads! In other words, the inability to rule-in VT does not rule-out VT! That's why these criteria are dangerous. In the absence of compelling evidence to the contrary (e.g., obvious sinus P waves in a 1:1 relationship with the QRS complex and a normal PR interval, an "old" ECG for comparison that shows identical QRS morphology, occasional pauses that reveal flutter waves), regular wide complex tachycardias should be considered VT. There is no algorithm that can safely classify a wide complex tachycardia as SVT with aberrancy.
-
You could go even further and say that the impulse originates in the area of the left anterior fascicle of the left ventricle.
Why?
What type of bifascicular block presents with an upright QRS complex in lead V1 and a right axis deviation?
RBBB and LPFB.
With RBBB and LPFB, which fascicle depolarizes first?
The left anterior fascicle.
-
For rhythm analysis, I like any lead that shows good P waves, QRS complex, and T waves. At least with a 12 lead, you've got your choice!
Tom B.
Alright Adam I waited enough.....I'm calling it V-tach. The right ward axis, wide complex (its completely ventricular in nature) lack of P waves, and rate in itself all show the rhythm.
Tom, wouldn't that suck major if no 12 lead was done on this patient? Lead II totally sucks in this one.
Every cardiac monitor defaults to Lead II, this just goes to show you, that you must not always think "inside the box". I'm a strong believer of not using lead II as a simple strip on the monitor, for this reason! Lead III and V1 are much much better.
-
No one is telling you to stray away from your protocols Fiz. You should do exactly what your medical director expects of you. Keep the combo pads nearby though. As for Tom's post, Amal Mattu is an emergency physician that has become a near expert in electrocardiography. He may not have it written down as a scientific method, but doing something that has shown no improvement but has shown potential harm is lunacy. This is why the Trendelenburg position is soon to fall out of favor. AHA will be renewing their guidlines next year, I predict Amiodarone will be sitting in the backseat this time around.
Read this post on Ambulance Driver's blog, He explains the over use of "selective cardiotoxins".
My views on these types of topics are constantly changing. Five years ago, I wouldn't have had any idea what AF/WPW looked like, let alone how to treat it (or not treat it). I'm not a huge fan of prehospital antiarrhythmics in the first place. At least for regular wide complex tachycardia, you probably won't harm the patient by trying 150 mg of amio over 10 minutes. Of course, with AF/WPW you have the same concerns about symptom onset < 48 hours that you would have with any other AF. Like I said, I just don't care for prehospital antiarrhythmics, so I wouldn't feel comfortable monkeying around with AF/WPW. If it's unstable, I'll shock it. If it's stable, I'll let the ED physician (or a cardiology consult) figure it out. I wouldn't judge someone for giving amio since it's an option in the AHA ECC 2005 guidelines for irregular wide complex tach. I just wouldn't do it based on the possibility of causing harm with no clear evidence of benefit.
Tom B.
-
Absolutely, and no hostile or pointless argument is desired.
Thanks for the discussion!
Tom B.
I agree this is an educational discussion; however, people are going to disagree based on how they look at this XII lead. As I stated, I am not arguing against looking at this as ventricular until proven otherwise. However, I stated for the sake of mental masturbation, I am using axis as a tie breaker. We disagree on our assessments and go about our way without resorting to personal attacks, creating yet another hostile and pointless argument.In addition, where have I ever called my self "the great chbare?" Where have I sated that I cannot learn anything? Clearly, I am capabable of learning and have incorrect assessments, ideas, and concepts. Remember the paced rhythm strip tease? I initially missed that one. I am quite sure you can look at my other posts and find where I had the wrong idea or thought.
I considered his stance and think it is a sound one. However, I continue to disagree. We disagree, not a big deal.
Take care,
chbare.
-
Uh oh, Tom "The Guru" is here, and I mean that as a compliment. Lets hope he can help me teach these. I'm going to let this one go a little longer to get some more impressions.
Tell me why you think it is what it is, if you haven't.
I'm not a guru, Adam. Just a guy with strong opinions. Some of them might even be right!
Tom B.
-
There is this, and there is the AHA. I guess you need to decide which to believe, and follow your protocols. Neither this statement nor the AHA's is backed up with actual objective research, but that is because it doesn't seem like such research actually exists right now. In choosing between two sources of anecdotal opinions like this, paramedics probably should just pick the one that favored most in your local area. My protocols say to give amiodorone, so that is what I will do (if it can't be avoided).
In the absence of evidence that it helps, and with anecdotal reports of possible harm, why give it? Synchronized cardioversion is a perfectly viable option (and so is supportive care for hemodynamically stable patients). The first rule of medicine applies.
Tom B.
-
As ERDoc stated, debating the specific focus of the escape rhythm is academic when considering the pre-hospital treatment of a symptomatic patient. However, for the sake of mental masturbation, why not discuss the possible focus of the escape rhythm?
Again, I point to the axis. Right shoulder axis deviation is still suggestive of a ventricular rhythm; however, this patient clearly does not demonstrate right shoulder axis deviation. As people have stated, the right shoulder finding is not always the case; however, it still provides evidence against a ventricular rhythm.
As ERDoc stated, the rate is around 40, this is ~the upper limit for a ventricular escape (not including accelerated rhythms), and the ~ lower limit for a junctional rhythm. So, yes I would agree, it's a hard call when you have a wide complex escape rhythm with a rate that could go either way. In my case, I am using the axis as a tie breaker.
Take care,
chbare.
I don't see how it provides evidence of anything. Most cases of VT present with other than right superior axis. Why should ventricular escape rhythms be any different? In my world, wide complex rhythms are ventricular until proven otherwise, and rate, axis, and QRS morphology are not sufficient evidence.
Tom B.
-
I'm still curious to know how you differentiate between a junctional escape rhythm with LBBB and a ventricular escape rhythm. If wide complex rhythms are ventricular until proven otherwise, then you should consider this 3AVB with a ventricular escape rhythm. Or, 3AVB with a wide complex escape rhythm. There's no need to call it a BBB. Maybe it is, maybe it isn't.
Tom B.
-
Why do you say amiodarone is contraversial? It is the everything channel blocker (in essence) applying the breaks to the whole truck, and not just the front set of breaks...
Also, as for Adenosine, the drug card that comes packaged with Adenosine says that it can be used with WPW. Why do you say it will kill them?
Adenosine might work for an antidromic AVRT, but it's a risky drug that can trigger VF, especiallly in the setting of AF/WPW.
As for amiodarone, consider this transcript from Amal Mattu M.D.'s December 2008 podcast at EMedHome.com:
Another concern that you need to be aware of is, if you have a patient who has AF with WPW, stay away from amiodarone. Even now, AHA continues to list amiodarone as a viable option, but it’s not a viable option. In fact, the only published reports on using amiodarone in rapid AF and WPW have indicated that amiodarone is associated with adverse outcomes. There’s a handful of case reports of patients that had rapid AF and WPW. They got amiodarone and they decompensated. There are, to my knowledge – and I’ve looked through the literature in detail multiple times – and I have yet to find even a single case report or a single case series or a published study saying, “I had a patient with rapid AF and WPW, I gave him amiodarone, and they did well.” Not a single publication that I can find. The only publications on that particular scenario that have ever been published in the literature are "patient did worse" so my recommendation and a handful of other peoples’ recommendations also; "Stay away from amiodarone if you’re taking care of a patient with rapid AF and WPW." -
I like the answers being here, too. I'm going to guess it's an an accelerated junctional rhythm with a BBB. I'm not sure where the block would be, so I won't even go there.
My reasoning is that I see few if any p waves, but the rate is about 120-130 which is fast even for a sinus rhythm. I was going to call it ventricular(still might be) but I noted the "rabbit ear" and recalled that it was indicative of a BBB, and would account for the wide qrs.
Thanks for posting these. I'm learning alot! Just hope I'm not driving y'all up the wall in the process!

On a side note, the view from v6 was on one of our tests and was called v-tach but was represented as being from lead II. What kind of difference would that make as far which lead it's seen in? I don't even think I worded that right, as I know different leads look at different parts of the heart(we learned the SALI mneumonic) but I'm hoping you'll know what I'm trying to ask here. Also, in my effort to more fully understand, are the pt's symptoms more from the lack of atrial kick or from the decreased ventricular filling time? We were told that a rate under 150 usually didn't cause significant symptoms because while you'll have decreased cardiac output it's usually not much till you hit 150.
This is a good example of why we need 12 lead ECGs.
Can you imagine trying to diagnose this arrhythmia using lead II?
Yikes!
Tom B.
Regular, wide complex tachycardia at 120-130ish. This is either going to be VT or SVT with abbarancy. This one I think I would call VT because of the rightward axis (about +150 degrees, so not extreme right axis), and the reversed R wave progression through the precordial leads. Wide complex tachycardias are notoriously difficult to identify though, so I admit I could be wrong about this one.With the exception of hyperkalemia, you're never wrong to presume that a broad complex rhythm is ventricular! The burden of proof is on the person who says it isn't.
Tom B.
-
It is a LBBB, as the QRS is wide (its borderline at 0.12 sec), negative in V1 and the underlying rhythm is supraventricular in origin
Just to play devil's advocate, how do you know the rhythm is supraventricular in origin?
Tom B.
-
Also look at the axis. Right shoulder axis deviation is typically highly suggestive of a rhythm originating in the ventricles. Ventricular tachycardia, for example. For right shoulder axis deviation to exist, the QRS morphology in leads I, II, & III should demonstrate negative deflection. Lead I is clearly positive, so this rules out right shoulder axis deviation and most likely rules out a rhythm that originates from the ventricles.
I'd like to make a minor correction.
While a right shoulder (right superior) axis can be suggestive of VT, it's not true that rhythms with an other-than-extreme axis are unlikely to be VT.
With VT, you can have a normal axis, left inferior axis, right inferior axis, or right superior axis.
I apologize for nitpicking, but it's an important point.
Tom B.
Ventricular rhythms do not always present with extreme right axis deviation, be careful.Maybe I should have read through all the comments before I hit reply!
Tom B.
As a final thought, whenever the shortest R-R interval is 6 small blocks or less, there's an excellent chance you're dealing with an accessory pathway! My dept's protocols do not allow antiarrhythmics in the presence of delta waves, heart rates that = or > 250, or shortest R-R interval of 240 ms or less.
Tom B.
Prehospital Clearance of Spinal Injury
in Patient Care
Posted
If the patient has a normal level of alertness, a normal neuro exam, no signs of intoxication, no pain on palpation of the spine, no painful distracting injuries, and no pain with 45 degree lateral movement, flexion, or extension of the head, then no spinal injury exists. This is well supported in the evidence based literature.
The spine is a bag of bones, and it hurts when it gets fractured. I don't put every patient with a MOI in bilateral traction splints, and I don't put every patient with a MOI on a LSB.
Be a professional. Learn your job. Do it well.
Or, find something else to do.
Tom