


Jaymazing
-
Posts
65 -
Joined
-
Last visited
-
Days Won
1
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by Jaymazing
-
-
First off, don't worry about being older than your classmates. Life experience is vastly important in this industry, and you'll find that age will offer it's own particular benefits when it comes to communicating with your patients in the future.
Secondly, keep on 'nerding it up'! Enthusiasm is a trait that some of the more bitter, jaded folks in this industry might scoff at, but truth be told, this profession needs more people who are passionate about healthcare. Never lose that spark, and remember; find a job you love, and you'll never work a day in your life.
Welcome to the city, and welcome to our community. -
Because I work in the second largest gay community in the world (atlanta), so this is an every day or at least every week occurence for me. Sorry if you cant handle the truth.
I don't know where to start with this...
-
Thanks everyone for your comments!
Except for you, Mikeymedic. I don't know why you chose to comment at all, since dismissing the question and discarding other peoples responses is neither productive nor helpful to me. You clearly operate under a completely different set of personal guidelines than I, and while I'm sure you're MUCH smarter than me (you've clearly demonstrated that), I can in fact think of situations where this is pertinent information to have, and thus am admittedly still trying to improve upon my patient interview skills when it comes to broaching the more tender topics.Maybe where you work is different than where I work, but I can easily say that at least 80% of my calls aren't really "emergency settings" by most standards. And perhaps my tendencies to address my elders as "Sir" or "Ma'am" are outdated where you are.
But I'm supposing we live in very different worlds.
On a brighter note, I really like the bra-strap-auscultation idea, MariB, and I'm going to store that one in my toolbox for next time I need it!
-
1st of all congratulations. @nd of all u should have not thought of yourself as anything but human. I have had 12 continuos Pt. care at all levels I have never had that happen but always get a history a complete one if possible,
Welcome to the city.
I'm going to take a stab at deciphering this.
I think he was trying to be friendly, not condescending, but maybe I'm just reading it with a different shade of sunglasses (the writing is indeed poor). I think what he meant was first, "congratulations on the good call, and performing good patient care", then second, "We are all human. I've had 12 *years* of continuous patient care (at various levels) and never had that happen, which makes that even more impressive".
And then I think he was asking for a history, because he thought this was a scenario....but I'm being hopeful. Obviously a complete Hx gets put on the backburner when you haven't passed the 'C' of the ABC's.
I'm not ashamed to admit, I've struggled to find carotid pulses on people who I knew were alive. And I wouldn't be ashamed if I couldn't find one on someone who I thought was dead, either. I hope that nobody thinks that makes me a poorer practitioner, but if so I'd remind them that it's only when we acknowledge our shortcomings that we can truly improve upon them.
This sounds like a fun call, did you get to bust out Mobey's Magills?
-
 1
1
-
-
So, I'm sure we've all been in this situation to some extent at some point in our careers, and I'm curious to find out the best way to go about handling it.
Those patients who you just can't tell if they're a male or a female. How do you go about asking? Is there a polite way to do it? Maybe a subtle trick you use; perhaps in how you phrase questions? Or is it all about being blunt?
For the sake of eliminating a few of the obvious answers, lets say the patient is in their early twenties, average weight, doesn't have a wallet (and therefore no identification or paperwork), has a unisex name, is wearing bulky winter clothing, and has a voice that keeps you guessing.
The balls in your court. And yes, that was a pun, and no, I have no shame.
-
On slow days when we have EMT students, I like to get them to experience being strapped down on a spine board in a moving ambulance. It's a weird feeling, even for a healthy person, especially when the vehicle turns a corner. It certainly makes me feel dizzy, too.
Sometimes tilting the board for a while helps alleviate the dizziness, and as a plus you'll also be ready if the dizziness turns to nausea.
You can also try dimming the lights, that's worked for my patients in the past, but of course this is only really useful when you don't need the lights on. -
I'll take a stab at this! I'm just bouncing idea's around, so let me know if I'm out to lunch here.
Phosphaturia! And if I had to guess some mechanisms, maybe an increase in serum calcium 2ndary to the trauma and #'s, leading to increased excretion of phosphate, leading to milky urine output.
Or maybe the patient just drank a lot of milk or milk-based alcoholic beverages before their high-speed-collision. But that doesn't sound as cool as phosphaturia. Bailey's anyone?
As a side note, if you market "Mobey's Hybrid Selective Comfort Spinal Motion Restriction", I'd like to create a jingle for advertising. M-H-S-C-SMR rolls so nicely off the tongue...
-
I like jumpsuits for the simple fact that I don't have to keep re-tucking my shirt. I hate jumpsuits as soon as it's time to poop...I've put serious thought into implementing a "trap door" system on the back.
The 2-piece uniform on the other hand offers ease of access, and a traditional look that I like. But when one item fades in the wash faster than the other, and you end up having two different shades of navy blue, it's not what I would call "fashionable".
For me it boils down to what phase of the laundry cycle I'm at in my tour. -
I enjoyed this scenario, even though I didn't participate. It got a little sidetracked, but I learned stuff nonetheless
Thanks for sharing it!
-
I'm going to assume that since we can't get a head CT we also can get a chest, as someone mentioned a PE. Cxr is not helpful in diagnosing PEs (yeah you can see Westermark Sign or a Hampton Hump but those are usually only visible on the retrospectroscope). As cxr will tell us if there is heart failure, pneumonia, pneumothorax, an enlarged heart (possible pericardial effusion), or aortic aneurysm. Is is safe to assume we don't have a bedside US either? I'd like to get some labs going NOW. CBC, CMP, Trop, ABG, coags to start.
Chest Xray is negative for heart failure, enlargement, pnuemonia, pneumothorax, effusion, and aneurysm .
Ultrasound is not available.
There's some limit to what I can say for the labs, as I don't recall what they were! I didn't get to see them for more than a minute... But I also know how the scenario ends, so I can give you some idea what the results were (or would have been) to keep you on track. (I apologize for the lack of data here).
CBC will be within normal ranges, electrolytes are normal, creatinine and eGFR show slightly decreased renal function (nothing dramatic), Trops are negative, ABG was requested but never performed (actually). INR was slightly prolonged.
I don't want to make up the numbers, so I hope this manner of giving you rough answers will suffice for the sake of this scenario. I'll keep going as best as I can.
Can we get an ABG w/o a respiratory therapist?
We can certainly try! An ABG was requested at one point, but oddly enough no one seemed to do it!
How about D-Dimer? Would it be specific enough in this acute setting?
D-Dimer negative
Yeah, but if we don't do anything about the BP, seeing as he's missed his morning anti-hypertensive AND B-blocker, it's just going to keep going up and make the situation worse. I know hydralazine can cause tachycardia, but it also is very effective at lowering BP.
For sake of discussion, can you think of anything else you could use to bring down HTN in this situation?
What would you like to do for the rate?
Is there any other symptoms present that we can treat right now?
And the last Q to ponder; what came first? How did this cycle begin?
Hello,
Lots of reading to catch up on.
Once we clear up his level of intervention/code status I think intubation is a reasonable step. He has had a general decline in his LOC. If I recall, his GCS is around 8/15. He has respritory failure (oxygenation and ventilation).
Just for recap, Eyes remain closed, he is not answering questions, he withdraws from pain (and I should note, makes purposeful movements) but does not follow commands, and is making incomprehensible sounds (which isn't a substantial drop from the significant aphasia he had when you saw him yesterday). There is a decline in LOC that you can notice, but also a significant increase in distress.
If there are no indicators of a difficult airway or difficult BVM I think RSI would be the best method. Propofol and Roc.
There are some moderate signs of difficult airway, but you're a pro and I believe in you. Lets tube this sucker.
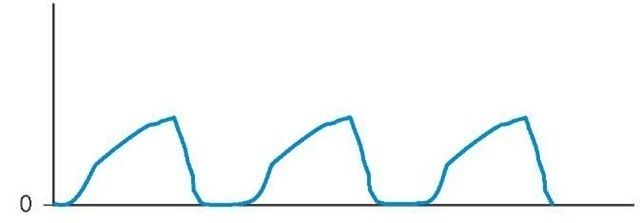
You visualize the cords, pass the tube, secure, confirm lung sounds bilat, and visualize waveform capnography that resembles this:
http://i3.photobucket.com/albums/y59/Jeyface/tmp2A94_thumb2221.jpg
As for the HR. I would get the airway done first and then see how the HR and BP play out. If the monitor is showing a rapid A.Fib post intubation a loading dose of Amiodarone and a ggts could be an option. Sure, cardioversion could be an option. But, this won't last until the underlying medical cause is managed.
Maybe, with some post intubation sedation and ventilation support the BP might come down some.
Snap a quick CXR when the tech gets in.
(see above)
Draw a ABG after 30 minutes or so to see how ventilation is going.
Sort out the logistics. As many poster have noted, perhaps CCT is in order.
Cheers
-
Are they monitoring his end-tidal co2 levels?
They have a nasal cannula with end-tidal c02 measuring on underneath the NRB, and it's picking up an ETCO2 of 32mmHg
-
So, he didnt get his am meds? Correct!
IV hydralazine for the pressure Would you give this as a front-line antihypertensive? Would the heart rate be of concern? Would you like to do anything about the tachycardia?
IV furosemide Done.
Stats cxr Pending. The technician is being called in from home.
Does this hospital have an ICU? Respiratory therapists? Negative on both counts!
Respiratory status likely due to not receiving his asthma, copd/asthma and chf. BP/HR likely d/t missing his AM beta blocker/antihypertensives. Very interesting! We should pursue this futher

Probably totally off on this, but it may stabilize him long enough to get a bird available or get a critical care team to ground transport to a ct hospital.
-
What/when was the last CBC, PT/INR? What rhythm does it look like at that rate? Any response to the adenosine? What dose of the adenosine? Possibility of cardioverting?
(See above for ECG)
CBC was normal, PT/INR was within normal ranges, Adenosine failed to cease the tachycardia, doses were 6mg and 12mg respectively, and you tell me if there's a possibility of cardioverting...do you want to cardiovert right now?
Why are there no physicians in the room??? A RRT should have been called and a stroke alert at the first notice of change in symptoms...but I'm guessing this is a small hospital with no such resources which brings me to the question of why in the world would he be brought back to podunkville just 48 hours after tPA?!? He should have been in a major hospital with CT capabilities...
The physician is currently at the nurses station, on the phone. You are correct in guessing that this is a small hospital. The attending physician is only 1 of 2 working in the community today, and they are also dealing with a chest pain patient in the emergency department as we speak.
As a meager minion of our healthcare system, I can't really say why the patient is back in podunkville so soon. I agree, he should be somewhere with CT capabilities, but sadly, he is not. So goes life in Podunkville, some days.
On to care....
I'd like to get that BP down, so like IV beta blocker to get that pressure and heart rate down...
What would you like to give?
Anyone else feeling like RSI and knocking this patient down for a bit? With the O2 saturation decreasing and his altered LOC, I'm not too happy with him controlling his own airway as he's stroking out and possibly going to code on us with a BP and HR that high.
Is there anything else you'd like to do/ask/know before pursuing the RSI route?
He's likely having another ischemic stroke (doubt hemorrhagic d/t pressure)... What meds is he on? What have his vitals trended?
Meds include several antihypertensives, beta blockers, lasix, ventolin/atrovent MDI, spiriva MDI, budesonide MDI, levothyroxine, ativan PRN, desvenlafaxine, ASA, acetaminophen, and some more that i unfortunately cannot recall.
He is normally poor compliance with his meds at home.
Vitals have been increasingly tachycardic, tachypnic, hypertensive, sats were initially 96% this morning (about 3 hours ago) and have been coming down since. If you'd like more specific numbers, I can try to track them down.
ETA: Any presence of corotid bruits? Patient Temperature?
Negative for carotid bruits. Temperature is 37.5 celcius.
You said the heart rate on the monitor is 190...what is it on his wrist?
Too fast to count, but it seems to correspond with the QRS complexes on monitor.
Bounding, grossly irregular.
Hello,
First, thank you for posting a scenario.
It is a little crazy that a CVA patient was transfer back to a small community hospital from the stroke centre so fast.
I concur!
Thrombolytic CVA can convert to a hemmorrhage hemorrhagic at the 24-48 hour mark. Basically, the ischemic tissue dies and a bleed can result. This is the same reason the ischemic changes do not show on a Head CT for the first 24 hours. This could explain the new neurological finding and the HTN.
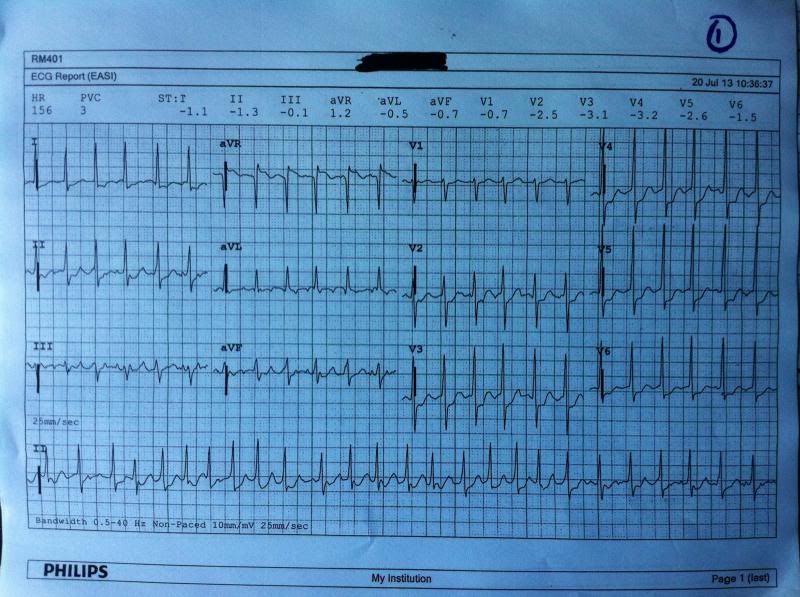
HR=190 What dose the monitor show?
http://i3.photobucket.com/albums/y59/Jeyface/ecg/photo1.jpg
Also, what is the code status/ level of intervention?
There is no advanced directive for this patient. But I'm glad you asked!
lastly, this is not a BLS transfer.
I concur again!
Thank you,
Thank you!
Well... hopefully you can cancel from the job since the patient has deteriorate but is in hospital and it’s not what you’ve been called for… If they want your involvement then:
Is he maintaining his airway? If not, triple airway manoeuvre and OPA as primary intervention. I’d like to provide positive pressure ventilation with an SP02 of 91% on high flow oxygen with a GCS of 8.
He is maintaining his airway, but its very labored. But he resists the BVM. Would you like to try anything else?
What are pupils doing? ERL, 4mm
What’s happening on ECG? Are they giving adenosine for SVT? http://i3.photobucket.com/albums/y59/Jeyface/ecg/photo1.jpg
What’s BGL doing? 9.7 mmol/ml
I’d like bigger IV access than a 20g at this stage. Done. 18g in the opposite forearm.
A total summary of IV fluids. Total of 150ml normal saline today, running at 75cc/hr
Recent pathology results. No labs have been done today, but they were good yesterday!
Further respiratory status assessment, auscultation, skin colour etc.? Grossly laboured at about 30/minute, coarse inspiratory/expiratory wheezing in the apices with no entry to the bases, cyanosis to the lips
Were the doc?
Elsewhere
Can we get a better history on the situation, how long ago did the symptoms start, has there been a rapid deterioration, what treatment has the patient received since being admitted to the rural hospital including what the nurses have done since the patient started to deteriorate? I’d still like to get a full past history and list of current or new medications.
Today when the nurses came in to administer the patient's morning meds (approx 3 hrs ago), they found that the patient wasn't swallowing and appeared to be increasingly agitated and not responding to questions. They moved the patient to a bed with telemetry and initiated an IV and NRB, and began organizing ground transport to a facility with CT capabilities. The nurses say that the symptoms came on gradually at first, then dramatically got worse when the family arrived to visit her this morning.
PmHx includes HTN, A-Fib, Hypothyroid, asthma/COPD, CHF, depression/anxiety, arthritis, and obesity. He reportedly has very poor compliance with his HTN and AFIB meds.
Meds include several antihypertensives, beta blockers, lasix, ventolin/atrovent MDI, spiriva MDI, budesonide MDI, levothyroxine, ativan PRN, desvenlafaxine, ASA, acetaminophen, and some more that i unfortunately cannot recall.
Treatment is really dependant on what your skills level is and what the hospital can provide?
I concur.
Sounds like the patient will need to be intubated…
So question.... why would this be hemorrhagic vs ischemic? Just based on the history of tPA? I didn't think you would see a BP THAT high with hemorrhagic. I'm not really seeing any signs of cushing's triad either indicating to me that the ICP isn't rising as it would with a hemorrhagic right?
Very good point
I'm just trying to work my brain on this one... I just have a very narrow experience with strokes so understanding more of the pathophys of all this can only help? Sorry

dont apologize! this is how we learn!
I'm glad you're participating
I would like to ask why you did this as a BLS Transfer. Most of us have stated that BLS would not be transferring this pt. and if ALS was not available I would be taking a Doc on car with me.
Personally with this pt I am picking up the air vac crew and be the taxi driver along with being extra hands if need. I am not touching this pt. with a ten foot pole.
It was dispatched as a BLS transfer, but as I'm sure you know, dispatch information can vary immensely from actuality.
Unfortunately, air medevac is not available.
You're more than welcome to be an ALS provider in this scenario. I apologize for not making that more clear in the initial information.
BLS transfer. Im AMFYOYO. In a ALS crew. Granted we have suspicion for another stroke but im rather curious if this is a possible pulmonary embolus. Chest x-ray would be nice to rule that out real quick. RSI and place on vent to bring up the SPO2. Initiate a second IV 18 ga or largest possible set to TKO. What was the result of the initial attempted cardioversion. Did it rhythm change after the initial dose of adenocard. After the intubation did the SPO2 improve. If nothing improves than request for a medevac. 2 hours is way too long for a patient in that condition and is still deteriorating.
I wish I knew what AMFYOYO meant haha
I like the diffDx! get those gears turning.
Adenocard administration showed brief asystolic pause, no flutter waves visible, with prompt resumption of tachycardia. This was the same for both 6mg and 12mg doses.
And I'll let you intubate, but you may wish to review some of the new information first.
-
First and foremost, I have to apologize for the incredible delay in me getting back to this scenario! I wont make excuses, but I've had a very interesting week to say the least.
But without further delay, Getting back to it!
For those requesting ECG's, I have several for you.
Following an initial 6mg, followed by 12mg Adenosine administration, this was the rhythm. No flutter waves were witnessed.
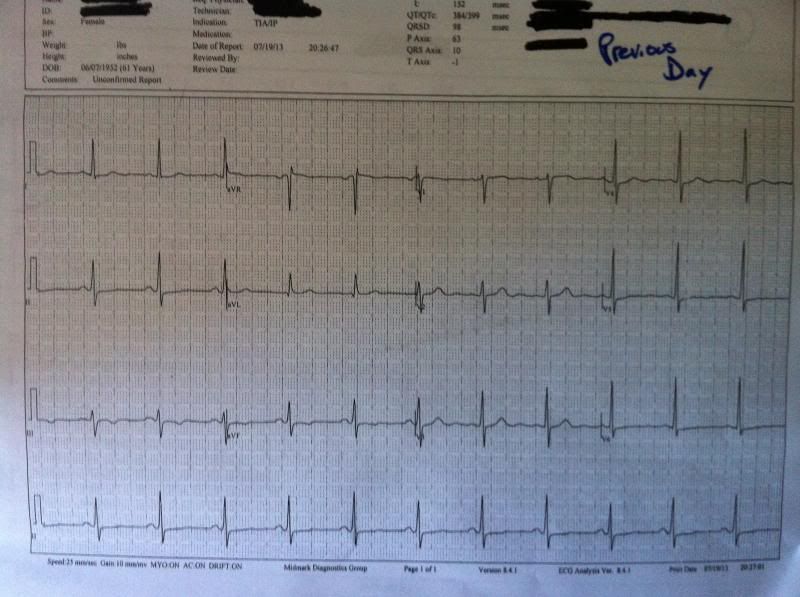
http://i3.photobucket.com/albums/y59/Jeyface/ecg/photo1.jpgFor anyone who might want to see an ECG from yesterday, you don't even have to ask....
http://i3.photobucket.com/albums/y59/Jeyface/ecg/yesterday.jpg -
I'd like to just note; it's a BLS transfer, but you don't have to be a BLS crew if you don't want to be. It's a scenario! Let's have some fun!
-
Well, I'd like him stable before I consider transporting bls. A wise decision!
What's him bp. O2 before and after the non rebreather. BP is 198/124, SpO2 on NRB is 92% and decreasing. I, unfortunately, do not know what the RA Sp02 was.
The ct is 1.5 hours away. Have they even done one yet? Before the TPA was given? After? They completed an emergency headCT prior TPA and ruled out hemorrhage. There was no tumor or mass. There was no repeat CT scan completed.
How is his conscious level? Not opening his eyes, not answering questions, withdraws from pain on the left, making incomprehensable sounds.
I think he needs a bird, not a bls crew Unfortunately, there's no option for flight right now. The heli and fixed wing crews are already on other runs.
-
You'll have to excuse the typos. For some reason I'm not able to go back and fix them....I dont have permission.
-
You and your partner are working in a rural community, about 2 hours from any major centersYou are called to your local health center for a BLS transfer of a 60 year old male, going for a Head CT. It's a patient you've already been acquainted with, since two days ago one of the other crews brought her to the nearby stroke facility (~75 km away) for a suspected CVA, and after being given TPA and receiving 24hrs of monitoring, you and your partner brought her back for continued care.It's been ~48 hours since TPA was given. Thrombolytics were unsuccessful, and the patient was left with right-sided paralysis and significant aphasia (he can only say "Yes", "No", and something that sounds like "bipisa").When the nurses came this morning to give the patient his AM meds, the patient was found to have lost the ability to swallow or chew (new finding), and seemed increasingly confused. The attending physician has now requested a repeat head CT at a center ~1.5 hours away.When you arrive at the nurses station to receive a report, you find that all of the nurses are missing. When you look around, you discover that all of the nurses are in the room where your patient currently is. They're moving around frantically, and they've just finished administering adenosine.The patient appears significantly distressed, is not responding to questions, and appears acutely ill. He's on a NRB at 15 lpm, has a 20g IV in his left wrist running at 75 ml/hr, and has cardiac monitoring showing a rate of ~190bpm.What would you like to know? What would you like to do? What do you think is going on?
-
It's called Laziness Jaymazing, pure laziness.
By golly, I believe you're correct!
One of the most advanced cases I've ever seen in my career. The prognosis is grim...Unfortunately, the best treatment is still prevention.
Open and shut case, my good man
-
This isn't even a question worth cheating on.
Seriously? You've picked the wrong profession if you can't do this on your own
-
First off, congratulations and welcome to the industry!
Secondly, advice for school.
I'm going to have to agree with the people commenting before me; if you can, get anatomy & physiology down, and to add to that start brushing up on your introductory pathophysiology.
My next piece of advice, don't let anyone take away that spark you have! You're motivated and passionate, and for the rest of your career you're going to have bitter, jaded, crusty old medics try to make you as bitter, jaded, and crusty as them. Fight the power, rock and roll, and keep on trucking in the free lane, my friend.You'll do great in school, as long as you continue to love what you're learning. Good luck
-
1
-
-
I'm in the same boat as Island, Dwayne, and Mike.
If it were me, I'd rock a shirt+tie with dresspants, and the jacket I'd have to play by ear depending on my understanding of the company I'm applying for.
I'm glad that you're so passionate about being seen in a professional manner. Our industry needs that.
Good luck on your interview. Rock and roll.
-
Happy Canada day, indeed!!!
-
i must have missed the point where anyone said anything about going against medical direction or protocol.....
That's okay. Won't hold it against ya, bud.
{kind=link}
{kind=link}
{kind=link}
50 y/o Chest Pain trouble speaking between breaths
in Education and Training
Posted
ABC's, general impression, and oxygen. Let's start finding out whats going on and how it all started?
If I have enough hands, I want a set of vitals and a 12-lead, too