


EMS_Cadet
-
Posts
59 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by EMS_Cadet
-
-
You could approach this from two perspectives...
First off, I need to see a 12-lead from this pt for further evaluation.
1). This appears to be a 2nd degree AV block type II with 3:1 conduction ratio. However, this type of block almost always originates in the bundle branches which would widen the QRS (not present). So the possibility is present for type I block.
2). You might be able to force 3rd degree AV block on this, but it seems that the third P wave in each cycle does conduct. 3rd degree block is usually wide as well unless you have an escape at or above the AV junction. I just don't see av dissociation here either.
My two cents...
-
http://www.wakegov.com/NR/rdonlyres/2F6EC7...0/2007Adult.pdf
Protocols are above.
This is our breakdown:
10gtt/set and a 250mL bag of NS.
Inject 12mL of epi 1:1000 into the bag of NS.
You can choose either 1mg/3min or 1mg/5 mins.
Also, if you look in the protocol, we also use epi drips in symptomatic adult bradycardia.
Let me know if you need any further.
-
We currently have epi drips in our cardiac arrest protocol as a standing order.
-
We can use the orange button (see post above) or we can say "Signal 25".
-

Your 12 lead is above.
-
Is there a possibility he was exposed to, inhaled, or ingested a poison or drug? What does he remember immediately preceding his symptoms? Is he telling you the truth about everything?
Double check BGL. Enlist ALS if available.
No toxic exposure or overdose. He remembers running around trying to catch his friend when pain started in his left arm and started moving down into his chest.
-
Respirations @ 28 and labored.
-
He is tachypneic with shallow respirations. Lung sounds are C/E bilat.
At this time, he is A/O.
-
S - Nausea/vomiting (new symptoms), "pain all over", dizziness, "faint feeling"
A - NKDA
M - Insulin
P - IDDM
L - Lunch (it's now 4pm)
E - See original post.
Vitals: Pulse @ 62, BP 92/68, Pulse ox @ 89%, Temp @ 98.7F. His skin is very pale, cool, and somewhat diaphoretic.
-
You are dispatched to an upscale neighborhood for a "DIABETIC EMERGENCY". Dispatch advises that your patient is a 15 year old male, known IDDM, with a chief complaint of "dizziness".
You arrive on scene. Scene is secure.
The mother lets you in the house and directs you upstairs to her child's bedroom. As you climb the stairs, you obtain that the child was fine this morning (it's about 1pm now), but was playing in the backyard with friends when he came in and started complaining of "pain all over his body". Mom assumed this was some type of neurological disturbance due to the diabetes. She checked his BS and it came back @ 156. She gave him some Motrin and sent him to bed. About 4pm, she went in and checked on him. He is now pale and cool. He is unable to move to due being extremely lethargic.
Go for it.
-
Hmmm...Very interesting scenario!
I'm very tempted to think that this is acute pulmonary edema. I am, however, reminded that no patient is "normal" or "textbook". As an EMT (and EKG guru) waiting to state test, this is my line of thinking:
More than likely, this patient has suffered a previous anteroseptal MI, causing acute heart failure. The presence of the Q waves in the septal and anteroseptal leads leads me to believe there was an old infarction. Also, since the bundle branches are contained in the septal area, an old infarction could possibly damage the LBBB. The septal damage is probably causing LV dysfunction, resulting in acute pulmonary edema.
As for the presentation, it sounds like a classic CHF case with the exception of the BP. However, this patient could be one of those "odd" people that has a fairly normal BP even during a major cardiac event. Also, does the patient have any edema, JVD, or abnormal cardiac tones?
I also would LOVE to get a BGL on this man. I don't think anyone has asked for one, despite his NIDDM.
I said it a while ago...Honestly, I wasn't thinking a valvular issue, but it did cross my mind.
-
Hmmm...Very interesting scenario!
I'm very tempted to think that this is acute pulmonary edema. I am, however, reminded that no patient is "normal" or "textbook". As an EMT (and EKG guru) waiting to state test, this is my line of thinking:
More than likely, this patient has suffered a previous anteroseptal MI, causing acute heart failure. The presence of the Q waves in the septal and anteroseptal leads leads me to believe there was an old infarction. Also, since the bundle branches are contained in the septal area, an old infarction could possibly damage the LBBB. The septal damage is probably causing LV dysfunction, resulting in acute pulmonary edema.
As for the presentation, it sounds like a classic CHF case with the exception of the BP. However, this patient could be one of those "odd" people that has a fairly normal BP even during a major cardiac event. Also, does the patient have any edema, JVD, or abnormal cardiac tones?
I also would LOVE to get a BGL on this man. I don't think anyone has asked for one, despite his NIDDM.
-
I didn't say anything specific about Plavix. People were asking about his meds and that was one of them. Then someone asked if he was still on it. It might mean nothing (or it might mean everything).
EMSCadet, I will try to answer all of your questions:
No exposure, no ingestion as far as the nurse knows. The pt is bed bound and has not fallen. The only ones to visit have been several family members (2 sons, a daughter and a brother). Pt was last seen the night before. He does not self-administer meds. No recent surgeries. The nurse has only known this pt for 3 days and he is not any different from when he arrived. There is no family present. Airway is patent and the pt is breathing and maintaining his sats. There is a weak but palpable radial pulse. No signs of trauma. There is no cyanosis or edema. You are unable to perform orthostatics on the pt. No hives or rash. The pelvis is stable. He is incontinent of both stool and urine. Abd is soft, nontender without masses. Vitals were already given. He can only answer yes/no and when you ask him if he is having any pain, he indicates no.
Alright...Well, I'm gonna admit that I'm sorta lost. Possibly a seizure (his mental status might be from being postictal)? CVA is still in my list.
-
Please forgive me, but I'm gonna have to start my assessment from the beginning. It's too confusing for me to "skip" over certain parts that have already been answered.
Alright, let's give this a go.
-Scene Questions
- Any exposure to toxic gases/hazardous materials?
Any possible ingestion of unknown substances/medications?
Any known falls?
Last time patient was seen?
Has the patient complained of anything recently?
Does the patient take his medications or does the nursing staff administer them?
Any recent visitors?
Any recent surgery?
Has nursing staff or fellow patients noticed the pt. acting out of the normal?
- Mental Status?
-Airway-
-Breathing?
- -Adequate?
-Any signs of poor oxygenation?
-Circulation?
- -Any obvious bleeding?
-I'm assuming a (-) radial pulse?
-Skin color/temp/condition?
-Rapid medical exam.
- -HEENT - Any edema? Pupils? Nasal flaring? JVD? Tracheal deviation? Hives? Cyanosis?
-Chest - Equal chest rise and fall? Any paradoxical movement? Breath sounds?
Heart tones? Hives?
-Abdomen - Any tenderness, ecchymosis, guarding or masses? Hives?
-Pelvis - Stable? Incontinence?
-Lower extremities - (+) PMS in both? Any edema? Hives?
-Upper extremities - (+) PMS in both? Hives?
-Any signs of trauma?
-Vitals
BP, HR, RR, Temp, BGL, Pulse ox, Co2. Orthostatic?
-Monitor: 12 lead.
-Cincinnati Prehospital Stroke Scale?
-SAMPLE history.
-Is the patient complaining of anything himself?
Alright...This could be anything, but my differentials include (but are not limited to):
-MI.
-Shock
- -Cardiogenic.
-Anaphylactic
-Septic.
-Neurological.
-Hypovolemic.
-Neurogenic orthostatic hypotension
-CVA (rare, but maybe).
-Post-ganglionic sympathetic denervation (I came up with this after some research on Parkinson's and hypotension).
-Pulmonary embolus
-Medication effect /overdose
-
Onset (time, sudden/slow onset)?
SPO2?
Associated symptoms? (chest pain)
Has this happened before?
BGL?
Has she taken her MDI for this event?
Are the MDI's empty or expired?
Air entry sounds?
Smoker?
Is home O2 on and working to cannula?
K thats enough for now!
SpO2: 92% on 2LPM via NC (home oxygen therapy).
Onset: The patient was eating, got done, and decided to watch some TV. The dyspnea started while watching TV.
Associated symptoms: Weakness, upset stomach.
Has this happened before: "Not really, I just can't catch my breath."
BGL: 102mg/dl.
MDI: Positive use...Three albuterol treatments...No relief.
Breath Sounds: Superior - Slight wheezing. Inferior - Rhales.
Smoker: Used to be, not no longer.
Everything is good with the home o2.
-
You are dispatched to a respiratory distress for a 82 year old female.
You arrive at a assisted living facility. A family member greets you at the door and directs you to the patient's apartment.
Upon arrival to the patient's apartment, you see a elderly looking female appearing to have some slight respiratory distress. She is on home oxygen and you notice some MDI's on the table next to the patient.
Hx: COPD, IDDM, HTN.
Meds: Insulin, HCTZ, Benazepril, Ecotrin, and the MDI's for the COPD.
Vitals: 140/90. Pulse @ 92 and regular. Resps @ 24 and slightly labored. Skin is slightly diaphoretic, but otherwise pink and warm. Temp is normal.
EKG: NSR with no ectopy.
What else do you want?
What do you think is going on right now?
-
Hey all,
Quick question for all the medics here.
Tonight, we were notified that a family member was sent to the ER for chest pains via ambulance.
I spoke to the nurse who activated 911 and got the following.
83 year old female.
Hx. of diabeties, CHF, TIA's and other things.
The med list is about a mile long.
No allergies.
Vitals: BP- 100/70. HR - 67 Temp - Normal. Pulse ox - Normal. BGL - normal.
Chief complaint was chest pain with shortness of breath. I was unable to find out if the pain was radiating. The nurse did not get a pain scale.
From what the nurse said, the SOB was severe.
The nurse had orders to give nitro tabs for chest pain (as prescribed by her doctor).
The nurse administered (3) nitro tabs without relief.
The nurse took a BP again and it dropped a little (expected that with the nitro).
The nurse proceeded to tell me that the paramedics "hooked her up to the heart monitor and said everything looked fine." I then questioned the nurse if the paramedics preformed a 12 lead, she acted stumped and said, "I don't know." From what medics have told me, you can't confirm a STEMI in just one lead.

My question is...I thought you weren't supposed to give nitro to patients with a systolic <110.
Also, could CHF start off with this presentation? I thought CHF started off with hypertension and patients only presented with hypotension when they started decompenating.
Thanks,
BR
-
We have it in our protocols.
-
Let's not even think about the condom section...
-
You're kidding, right?
Shane
NREMT-P
Let's hope the person is kidding.... :shock:
-
Did you try vagal maneuvers before the adenosine, and if not...why?
We did....They produced no results.
-
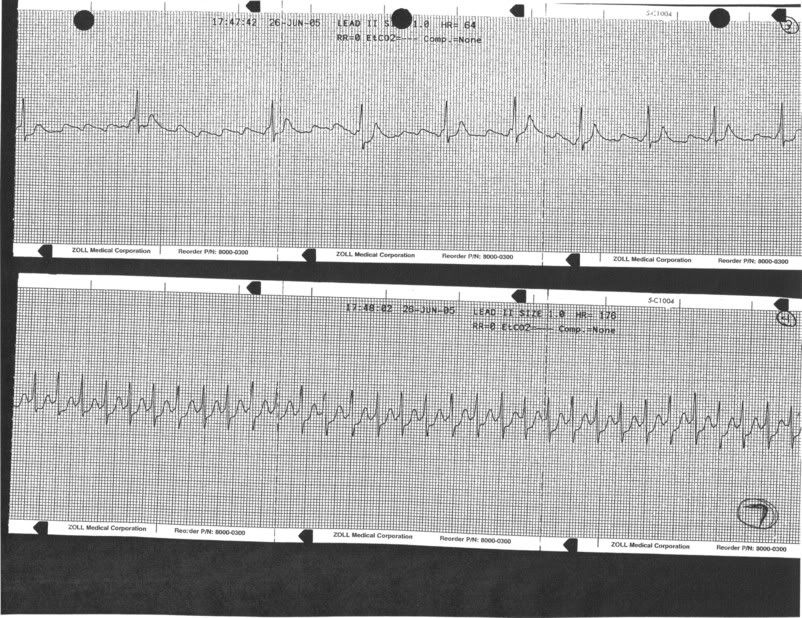
Alright.....
This is the rhythm after the 2nd 12mg. dose of Adenosine. (The 1st dose was also 12mg.)
The top strip is the rhythm at a slow rate. However, the Adenosine didn't seem to last to long because the rhythm converted to the bottom strip.
-
I agree, does this feel like palpitations or like her heart is pounding?
Looks like PAT (I can see P waves in the otherwise unremarkable 12-lead,). Even though I'll assume she has a Hx of afib (but it looks pretty damn regular rate aside), there is no WPW present.
We don't carry anything to give to that (unless you want to use adenosine as a diagnostic agent, which I don't think I would).
Technically she is an "unstable" tachycardia (Chest discomfort), but realistically she appears hemodyncamically stable (no CHF, everything else jives).
Has she been compliant with her diltiazem? How long has she been on it for?
Give ASA...Trial vagal maneuvers if you are comfortable, and trial diltiazem...She needs rate control.
Pt. has been compliant with her meds.
Anyone want to see the rythm at a slower rate?
-
See if that pie is done yet?..
I would also asked what position she was in checking the pie, bent over, carotid bruits, heart tones, etc.. of course as CHBare described, ECG, IV, FSBS, etc..
Have the describe the pain, sharp, dull, palpitations, associated with breathing, producible with pressure?.. It sounds more like palpitations..
How warm is the room, gas or electric oven?..
R/r 911
The pie is DONE!

She just bent over to check the pie. Nothing abnormal occured as she bent over.
This "funny feeling" started before the baking. She thought baking a pie would help. :roll:
Pt. states: "This is not a pain, but a funny feeling. It's quite odd. I had this several years ago, but I don't remember the name of the condition."
The pain does not change with inhalation/exhalation.
The room is normal in temp. Electric oven.
{kind=link}
Strip Tease 13
in Patient Care
Posted · Edited by EMS_Cadet
http://www.medicine.nevada.edu/dept/IMNort...SKulick_001.pdf
Page 5, third point.
"Almost always located infranodal (the bundle branches), which means that the QRS duration is wide."
I do see your point and it is quite valid. I suppose you could have either.
The AHA also makes several interesting points on their website..
"This type of block [Type II second-degree AV block] most often occurs at the level of the bundle branches."
"Conducted P waves may display a normal QRS complex if the site of block is within the bundle of His, or a bundle branch block pattern if it is more distal, as in the bundle branches, which is more common."