JMedic
-
Posts
7 -
Joined
-
Last visited
JMedic's Achievements
")
Newbie (1/14)
0
Reputation
-
ems is dispatched to a local supermarket for a patient with shortness of breath. ambulance paramedics arrived to locate a woman seated complaining of swelling to the face and trouble breathing. this patient has no known allergies and the only medication she is on is motrin with she took this morning without problems. patient also reports feeling light headed and dizzy. physical assessment is as follows: respiration rate elevated at approximately 24 to 30. pulse rate is 100 and weak in the extremities. blood pressure is low and 70 over 40. no significant ortho static changes noted. no cyanosis noted to the distal body or lips no hives or itching sensation noted anywhere on body airways open and self maintain skin is pale cool diaphoretic no bite marks or insect scars on body lung sounds are clear in all fields throughout treatment treatment is as follows: Ekg twelve lead nsr without ectopy. Spo2 low 80s room air 02 via nrfm 15lpm Pt placed trendelenburg on stretcher. ongoing assessment; with in approximately 15 to 20 minutes of ems care patient symptoms and signs diminish completely including shortness of breath. patience skin color improves in the blood pressure is up to 110 over 70 and pulse rate is strong in radial areas. what could this be? reminder :only treatment given by ems was continuous hi flow oxygen and monitoring patient has no significant past medical history. patient eats drinks and sleeps appropriately. blood sugar normal. Pt is post menopause. patient reports to have minor symptoms of constipation throughout the past 2 days but has no loose stool or excessive vomiting or any vomiting at all. extremity checks come back on remarkable 4 examination of poor vasculature.
-
I was going with either of your first two thoughts. Maybe a third Degree heartblock and the atrial waves are buried into the ventricular waves. And Idioventricular rythm was my second guess, but it kind of made be second guess that because of the QRS being so narrow. As for the Junctional Rythm, I don't want to focus on that too much because of the fact there are no definate, or indefinate P-waves, whether they be, positive. negative, or absent. Glad this has some people thinking.
-
94 year old female at home, AOx3, Blind, non-ambulatory, no orthostatic changes, Resps 18, BP 120/76. SPO2 99%RA, Medical Hx of one episode similar, which the hospital found was secondary to electrolyte imbalance, but never did anything about it, including no pacemaker, hx of CHF, L/S clear all areas throughout. Family reports that pt's urine has smelled foul the past couple of days. Not acting right, wanted her checked out. So I know possible factors of the rythm, but what is it that's actually DIRECTLY causing the rythm seen on the strip. Thanks guys. Hope That Helps.
-
CPR is never supposed to be paused if unnecessary. Actually, intubating someone and having stop CPR is unnecessary. If you're not lucky enough to get the ET tube while compressions are being done, go for a Combitube, or a King Airway, or some kind of Esophogeal airway.
-
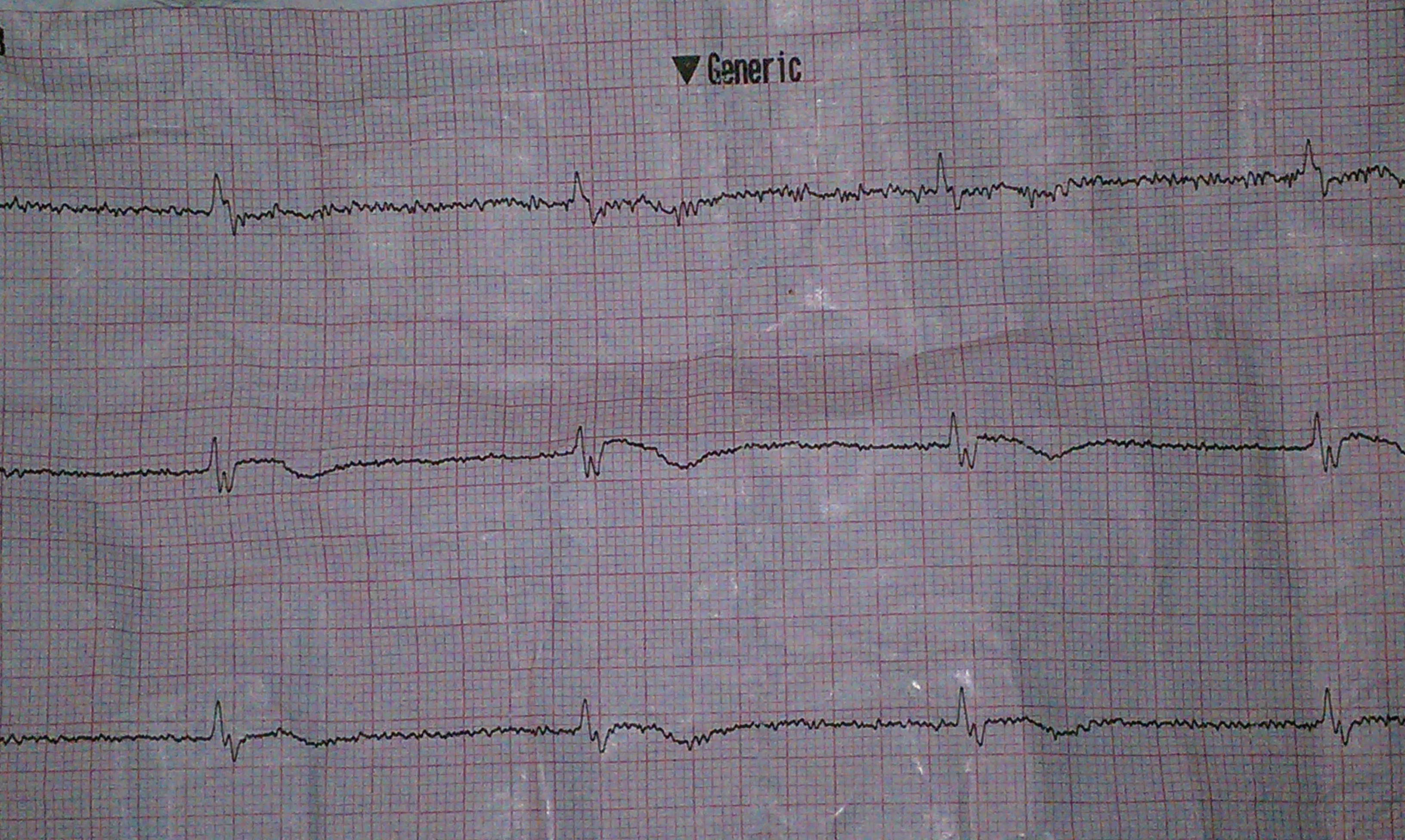
Here is the strip. Every once in a while there are some uncertain ectopic beats, but this ekg itself took hours to upload and im not bothering with the other one. Let me know what you think.

-
The Hudson Valley Region just re-approved, and effective immediatly, the use of turniquets. The deal is, you should apply direct pressure, and continuosly apply dressings to the wound. If this does not work, we use QuikClot dressings which absorb and "seal" up the blood leak, granted it's a vein or artery. If this does not work, we will now be allowed to place a turniquet closest to the laceration. We are allowed up to 2 turniquets be applied. Also, studies show no more elevating the legs, because the pressure from lower extremities push on the diaphram to labor breathing. Interesting what time and study will do.
-
Just looking for some input on a patient I had yesterday. We were dispatched to a residence for someone in a "weakened condition". We arrive to find a 94 year old feeling "tired". She was blind, and had a history of CHF. The vitals were stable,,except for the pulse. a 3 lead EKG was attached indicating a rythm of 36 and holding throughout. Upon recieving the 12 lead, there was narrow complexes, but no apparent P waves or anything else. You were able to determine notches in some of the complexes, but nothing else. Fluid therapy of 650cc's Saline did not work, and Atropine was not administered because of no certain P-waves. The patient was transported to a Heart Center 15 mins away where the ER had some trouble making out the rythm. I went with a form of heart block where maybe the P's were buried in the complexes, but I'm very interested in seeing whether or not anyone else agrees, or disagrees. I'm open for opinions. Thanks!