Arctickat
-
Posts
1,994 -
Joined
-
Last visited
-
Days Won
94
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Everything posted by Arctickat
-
Not sure where you're seeing AF Dave, however, I'll throw the last of the info that I am able to provide at this time. These are all we have available for labs, but were sufficient to make the diagnosis. We can't do Tox or ABGs. The PDF files of the lab reports can be downloaded from the downloads section here: http://www.emtcity.com/files/download/28-scenario/
-
-
File Name: Scenario File Submitter: Arctickat File Submitted: 16 Sep 2013 File Category: Misc Files Files associated with a scenario presented in the forums Click here to download this file
-
Not available at my facility.
-
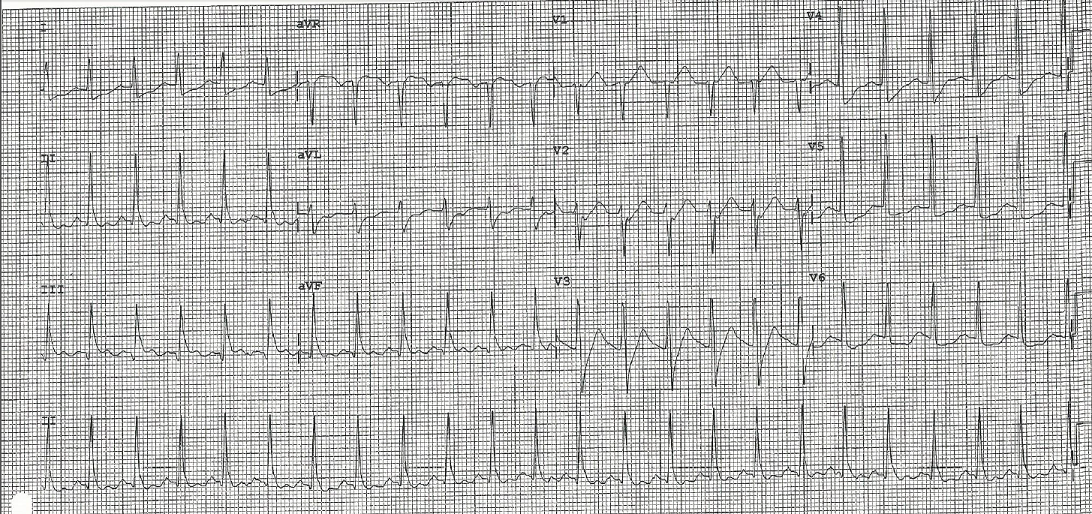
You've arrived at the hospital. Any thoughts to the underlying cause before I post the labwork? BP 127/83 HR 136 RR 14 spontaneous resps SpO298% on 100% O2 through the ventilator etCO2 36mm/hg Summary: Cardiac History AMI x 4 Diabetic History (Non Insulin Dependent) Prosthetic Eye Current untreated significant Infection Post Cardiac arrest ROSC after 15 min CPR and 1 defib 1mg Epi for Bradycardia PEA Intubated ECG Sinus Tach 5 mg Versed for Seizure Bilat IVs running TVO
-
IV Catheter -v- Finger Stick Blood Glucose
Arctickat replied to jwiley40's topic in General EMS Discussion
The only real problem is that the glucometer we use is calibrated for capillary blood rather than venous. However, as mentioned, the variance is so slight as to be insignificant to our treatment process. I will guarantee you that if you take your glucometer and poke your index finger on one side and then on the other you will get 2 readings that are 5% apart 9 times out of 10. -
3 minutes from the hospital you're congratulating yourself because your patient has been improving since you defibbed and is breathing on his own...when the patient goes into full tonic clonic seizures.
-
Given there is no comment we'll move along. Would you consider an amiodarone infusion? Why or Why not?
-
Nice call Triemal, Transport has begun Lung sounds are clear and equal, vent is hooked up. Core temp is 36.8 C No abnormalities noted, no discolouration besides the foot noted below, clothes are moist around the crotch No pacemaker The skin above the infected foot is red past the knee and the veins in the foot are red lines up the ankle. No response to pain, however there is some respiratory effort now. He was haying, no chemical exposure His left eye is a prosthetic. Client also has a history of Type 2 diabetes and Hypertension.
-
I see where you're going Jack. Interestingly enough, had I sedated this patient we would have missed a very important clue as to the underlying cause. So, we will hold the sedation for the moment. Summary: Client calls 911 for chest pain, past Hx of 4 previous MIs, and an infection for the past few days. Code status witnessed by EMS with CPR started immediately. Post resus after 15 min of CPR and 1 defib Pt is intubated ECG is Sinus Tach BGL is 22.8mmol/L Epi 1mg has been given 2 IVs are in place BP 132/70 HR 140 RR 12 with BVM SpO2 98% etCO2 39 Anything else you'd like done prior to transport?
-
NYS emt cert with felony conviction
Arctickat replied to gerald Jones's topic in General EMS Discussion
Well, given that you're a multiple offender without remorse, even if you do get a cert I would hope no one would hire you. -
Why would you need to sedate him with a GCS of 3? You don't need medical control to intubate an apneic patient. Edit: Pupils remain the same
-
Second line is in, BGL is 22.8 mmol/L, Lung sounds are good, Vitals are still good, with the exception of no respiratory effort, Would you like to intubate?
-
GCS is 3, 12 lead is attached Vitals: BP 132/70 HR 140 RR no respiratory effort, BVM and OPA 12 per minute SpO2 96% Skin, warm, pink, dry Pupils, Right ERL, Left Non reactive.
-
Epi is given and a perfusing heart rate of 130 - 140 soon appears with a BP of 128/67, Sp02 is 94 and climbing with BVM and an OPA.
-
Triemal; The ambulances met on the side of the road, no turnout is available. Both ambulances are the same size, just the cot mounts don't match up.
-
Okay, I misspoke, there is room for 1 more to get in and operate the BVM at the head. The Defib pads are placed and the first shock delivered. Pt converts to a 10 bmp Sinus brady on the monitor with no detectable pulse.
-
Would you take the time to switch the monitor over to yours or would you relieve the exhausted EMT and do CPR while he locates and places the pads for defib? The monitor also has the BP cuff and SpO2 connected.
-
Patient was working in a field and started having chest pain, he called 911 and during the call the 911 operator lost contact with him for about 2 minutes. The BLS crew were given incorrect directions and the BLS response ended up being 25 min. He was Alert and Orientated when BLS arrived and began transport. During transport he had a seizure which preceded the cardiac arrest. He has a history of 4 previous heart attacks and his wife says he has been planning to see the doctor about an infection in his foot. There is only room for you and the EMT in the ambulance and their cot won't fit in your unit. There is an AED in the ambulance with the 3 lead electrodes applied, but no therapy electrodes.The defib is a brand you're unfamiliar with, but it clearly shows VFib. Thanks Mike. I was never really away.
-
So, you're dispatched to intercept a BLS ambulance service enroute with a patient having chest pain. 1 minute into your response you're told the patient is in cardiac arrest and CPR is in progress. 14 minutes later you intercept the BLS ambulance and get into the back with the EMT, ECG is hooked up, OPA is in place and the EMT is doing 1 person CPR with the BVM....
-
Given that the nearest CT scanner to me is 175 km away and that there will be a 2 hour delay in transport while my local docs piss around trying to figure out what to do...an emergent response would be unlikely because we're less than 2 minutes from the facility. However, the transport to the CT scanner may be a different story if there is a high risk of internal bleed or any indication of altered mental status.
-
Welcome to the city. I haven't been to NAIT in over 20 years, but I'm sure nothing has changed. When in doubt, answer "C" and never review your exam after you're done writing it...studies show that people tend to change the answer and get it wrong.
-
Worlds first ambulance for kids launched in Dublin.
Arctickat replied to Leprechaun's topic in EMS News
Bless their souls, however the media needs to research this a bit better. What exactly makes this ambulance the World's First? I know of several pediatric ambulances that are very similar in capability. -
Head injury + Warfarin (Coumadin) = CT scan for Sub Dural bleed.
-
My dad never had CABG, but did get 2 angios done on a total of 5 arteries. Kept working for years afterward.